
Nuclear Families: A Social Study of British Nuclear Test Veteran Community Familiesby Dr Becky Alexis-Martin, Dr Emma Waight and Dr Mwenza BlellFinal Report: May 2019
|
![]()
This study was funded by the Aged Veterans Fund (AVF) by the Chancellor from Libor Fines through the Nuclear Community Charity Fund (NCCF) which was initially a Subcommittee created by the British Nuclear Test Veterans Association Charity 1131134 (Old BNTVA). In 2017 the NCCF was established as a Charitable Incorporated Organisation No1173544, the Old BNTVA became defunct and transferred its remaining assets to a new Charitable Incorporated Foundation The British Nuclear Test Veterans Association 1173575 (New BNTVA). In 2018 The AVF became part of the Armed Forces Covenant Fund Trust (AFCFT)
This document and trademark(s) contained herein are protected by law. This electronic and physical representation of University of Southampton and NCCF intellectual property is provided for non-commercial use only. Permission is required from Dr Becky Alexis-Martin, the University of Southampton and the NCCF to reproduce, or reuse in another form, any of our research documents.
The University of Southampton is a non-profit research and education organization providing objective analysis and effective solutions that address challenges around the world. The University of Southampton’s publications do not necessarily reflect the opinions of its research clients and sponsors. This report has undergone limited review and may be updated, corrected or adapted in the future.
© Copyright 2019 Dr Becky Alexis-Martin, The University of Southampton, NCCF.
All rights reserved. No part of this any of our research documents may be reproduced or reused in any form by any electronic or mechanical means (including photocopying, recording, or information storage and retrieval) without permission in writing from Dr Becky Alexis-Martin, the University of Southampton and the NCCF.
Published 2019 by the University of Southampton and NCCF
University of Southampton URL: www.soton.ac.uk
To order this document or to obtain additional information, please contact:
Dr Becky Alexis-Martin at b.alexis-martin@mmu.ac.uk
Executive Summary
Nuclear Families: A Social Study of British Nuclear Test Veteran Community Families
The Nuclear Families study has explored the lives of the UK atomic veterans and their descendants through questionnaires, semi-structured interviews, oral histories, workshops, participant-led events, participant observation, demographic analysis and archival research from 2016-2018. These approaches provided a snapshot into the current lives of this community with specific insights into their past experiences, present situation and future needs.
The Nuclear Families study has encompassed cross-generational experiences of disability, contested diagnoses, unmedicalised and somatic conditions; mental health and wellbeing, gendered challenges, cross-generational perceptions of hereditary risk, descendant reproductive decision-making and genetic altruism, memorialisation and death, ageing and hidden intergenerational care needs, and the influences of a historically minimal health and safety culture upon veterans today. This study identifies that there is still a diverse range of issues within this community which create a need for further support. The descendant community experiences trauma from perceived risks, and there are issues arising from mental and somatic health challenges. It also demonstrates the considerable support which is currently provided by non-governmental sources, with credit to the committees of the New BNTVA and the NCCF for facilitating remembrance, social events and community support.
This study recommends that the families of UK atomic veterans are provided with a specialist counselling service to support their understanding of their experiences and the likelihood any risks. This study also recommends greater specialist signposting for NHS professionals on the challenges arising for the descendants of UK atomic veterans; including autoimmune conditions, mental health challenges and addiction issues. A suggested NHS information template is provided in Appendix A for this purpose.
Contents
Nuclear Families: A Social Study of British Nuclear Test Veteran Community Families
1. Introduction to Nuclear Families 1
1.1 Why is Nuclear Families research needed? 1
1.4.1 Cohort recruitment and study overview 17
1.4.2 Semi-structured interview and questionnaire 20
1.4.4 Participant observation methods 22
3.1 Veteran health and safety culture 47
3.2.1 Contested diagnoses and un-medicalised conditions 58
5. Perspectives on Family Planning and Reproduction 71
7. Memorialisation and Death 79
8. Conclusions: Looking to the Future 87
Appendix 1: NHS information card template 91
Appendix 2: “’It was a Blast!’—Camp Life on Christmas Island, 1956–1958.” 95
Appendix 5: Participant Information Sheet Participant Information Sheet 107
Appendix 6: Participant Invitation 109
Appendix 7: Semi-Structured Interview and Questionnaire 110
Appendix 9: Ethics sub-committee application form 116
Appendix 10: Further Outputs – Talks and Presentations 125
References and Bibliography 135
List of figures
Figure 2: The benefits of focus groups vs. interviews vs. questionnaires (adapted from Harrell and Bradley, 2009). Error! Bookmark not defined.
Figure 3: Ethical Approval Checklist, University of Southampton, 2016. 25
Figure 4: Proportion of questionnaire respondents by response mode, n = 230. 27
Figure 5: Gender of questionnaire respondents, n = 229. 28
Figure 6: Age of questionnaire respondents, n = 229. 29
Figure 8: Marital status of nuclear test veteran descendants, n = 162. 30
Figure 25: Respondent identification of support resources (n = 198). 44
Acknowledgements
The Nuclear Families research team would like to thank the AVF, NCCF, NZNTVA, NAAV, Old BNTVA, New BNTVA and FNTVA. We also thank Professors David Martin and Graham Moon for their kind support in Health Geographies research, and for directing the study at the University of Southampton. Special thanks to Miss Fiona Bowler for her support with exploring nuclear test veteran health and safety culture using prior data collected by Dr Becky Alexis-Martin as part of this project, and for her archival research. Extra special thanks to Miss Ana Lorena, Mr Ron Watson, and Miss Susan Musselwhite for their academic and participant support with data collection at BNTVA events and beyond.
This report has been predominantly compiled using data that has been collected for the specific purposes of this project. However, we would also like to thank all of our many archival resources and supporters, including the archivists of AWE Plc, Los Alamos Nuclear Laboratories, the British Archives and the Hansard Collection.
This report is dedicated to all of the partners, wives, daughters, sons and grandchildren of the British nuclear test veterans; and of course, the British nuclear test veterans themselves.
-
Introduction to Nuclear Families
Nuclear Families is an interdisciplinary qualitative social sciences study of British atomic veteran families and their lives. The UK atomic veterans are the men who undertook work pertaining to the British nuclear weapon airburst testing programme. This encompasses the first British tests on Montebello Islands in October 1952, to the US-UK tests prior to Partial Test Ban Treaty of the 5th August 1963. The long-term experiences of these men and their families were shaped by the conditions, risks and consequences of life in the nuclear military industrial complex. This has led to some unexpected health, wellbeing and care outcomes for the veteran community and their families. This section of the report clarifies the need for research into this topic, delineates project aims and objectives, and provides an outline for the content and structure of the rest of the report.
-
Why is Nuclear Families research needed?
This study is needed to understand the current outcomes of the British nuclear test veterans and their families. This includes family health and wellbeing, NHS awareness and support, perceptions of risk, hidden care, memorialisation and death. A key motivation for this study is to understand the extent and presence of health and safety culture during the British nuclear weapon tests, and how this has affected veteran’s perceptions of risk.
There is a known legacy of challenges pertaining to the reporting and maintenance of radiation protection measures, during the British airburst nuclear weapon tests of the 1950s and 1960s (Roff, 2004; IPPNW , 1991). This means that it is more difficult to identify nuclear test veteran families who may be more vulnerable to specific radiation-induced health effects, and that there is considerable uncertainty surrounding the nuclear test veteran communities’ perception of their own health risks (Tang, 2017). Many of the 20,000 British men who travelled abroad to test nuclear weapons were young and uneducated, and did not understand the scientific information that was provided to them during pre-test briefings. It is also notable that many of these men were undertaking National Service and were conscripted onto work with an occupational risk of radiation exposure.
Radiation protection measures were present, but not a priority, when the Manhattan Project developed the world’s first atomic bomb in 1945 (Hacker 1987). Approaches to radiation protection were originally developed for assessment of the modest levels of exposure resulting from nuclear medicine and small-scale experimentation. Therefore, Ionising radiation dosimetry was upheld in terms of maximum “tolerances” and “body burdens”, rather than protective minimum exposure thresholds (Langham & Healy, 1973; Jones, 2005). While the deadly short-term effects of nuclear weapons were evident, there was little understanding of the stochastic (long-term) effects of ionising radiation following the bombings of Hiroshima and Nagasaki. This attitude persisted during the British nuclear weapon tests of the 1950s and early 1960s, when health and safety were generically less of a priority (Makhijani et al., 2000). In addition to these challenges, a culture of secrecy has surrounded the design, manufacture and health effects of nuclear weapons. Secrecy has been necessary to protect national security, due to the complexity of nuclear weapon possessor state geopolitics. However, it can have harmful effects to those who exist within the military hierarchy, as they can grow to feel that they are denied knowledge and that “Nobody told us anything”[1]. This community has experienced disproportionate and inaccurate perceptions of risk as a result.
This study explores some of the most significant long-term impacts to the veteran community, extending and developing existing research pertaining to medical, social and cultural challenges (Trundle, 2011). The nuclear test veteran family communities are an under-studied group, and little is known about their culture, lifestyle and wellbeing. There is therefore a need to survey the current British atomic veteran family health and wellbeing, and to discern the effects of a different historic health and safety culture upon contemporary perceptions of health risk for both veterans and descendants. The study has been expanded from this original remit to include hidden care responsibilities, memorialisation and ‘good death’. The Nuclear Families study is introduced here by describing why this study is needed, clarifying the aims and objectives of the research project, and outlining the structure of the report.
-
Report Structure
Chapter 1 summarises the key research concepts, describes the purpose of this work and outlines the report structure. Section 1.3 includes a review of previous studies of British nuclear test veterans and similar international communities, and Section 1.4 provides a more detailed overarching qualitative wellbeing research methodology.
Chapter 2 describes the outcomes from the questionnaire portion of study of nuclear test veteran family health and wellbeing. It consists of ten sections: Sections 2.1 and 2.2 describes participant response by gender and age, 2.3 looks at marital status, 2.4 describes self-reported physical health of the respondents, 2.5 presents data concerning mental health, 2.6 describes self-assessment of welfare and wellbeing. 2.7 concerns lifestyle, 2.8 presents data regarding care responsibilities, 2.9 presents questionnaire data regarding perceived hereditary effects of the nuclear weapons tests, and 2.10 presents the conclusions we may draw from this data.
Chapter 3 discusses themes emerging from the interview portion of the study. Section 3.1 explores historic veteran health and safety culture. Section 3.2 provides insights into the prevalence and type of disabilities that occur in the study cohort and investigates the occurrence and nature of somatic-related conditions such as ME and fibromyalgia, and briefly explores their links to community anxieties and other health problems. Section 3.2.1 describes cohort experiences of contested diagnoses and un-medicalised conditions and contrasts their experiences with existing literature on this topic, investigating the processes surrounding genetic citizenship and contested environmental illness (Trundle & Scott, 2013; Mix et al., 2009). Section 3.3 explores mental health challenges with focus upon depression, anxiety and PTSD. Finally, section 3.4 provides insights into the quality and nature of National Health Service (NHS) support, and identifies some existing challenges.
Chapter 4 identifies intergenerational and gendered differences in perception of risk, and some of the outcomes that arise due to these perceptions. The concepts of genetic altruism and perceived hereditary risks are introduced.
Chapter 5 explores the participants attitudes towards family planning and reproduction, which has emerged as a key impact of the nuclear weapons tests for both veterans and their descendants.
Chapter 6 explores hidden care responsibilities within the cohort community. It considers who provides intergenerational informal care provision and the implications of this caregiving for both the provider and the recipient. It identifies a need for improved pathways to formal care for both aged veterans and their descendants. This section also provides insights into the gendered responsibilities of care and the challenges that currently face women.
Chapter 7 provides insights into memorialisation processes and the experience of death. Memorialisation is a key aspect of the experience of being part of a nuclear test veteran family, and the places, spaces and types of memorialisation that are undertaken by this community are explored.
Section 7.1 investigates the process in the UK and beyond and explores the meaning of historic and paramilitary artefacts in providing comfort to veteran family members. The significance of medal provision is also explored, reflecting upon benefits to mental health. Section 7.2 considers death and dying in the veteran community, a significant yet unexplored aspect of being part of an aged veteran community, and its intergenerational implications for family members.
Chapter 8 provides conclusions to the study and suggests pathways forward for the community through improved NHS awareness of the lives and health of the atomic veterans and their families, the provision of telephone counselling service, and the provision of a medal to veterans and veteran descendants for memorialisation purposes.
A glossary of relevant terminology is included at the end of this report.
-
Literature review
The experiences of the atomic veterans were shaped by the conditions, risks and consequences of life in the nuclear military industrial complex. A lax health and safety culture combined with a culture of secrecy has had a long-lasting impact upon these men and their families (Hacker, 1992). Although the veterans believe that it was the tests that posed the greatest risk, their work presented many other significant hazards. The climate and geography of the isolated places where tests were conducted had a profound effect upon the mental and physical health of servicemen, and basic living conditions worsened these effects. Health challenges beyond ionising radiation included industrial accidents, the extensive use of carcinogenic DDT on the troops, poor sanitation, dysentery, severe sunburn, and inadequate rations (Alexis-Martin, 2019; Oulton, 1987). The way that these risks were faced and managed has shaped the veteran’s understanding of their time working on nuclear test series. Despite governments’ assertions that the nuclear tests had little or no risk of radiation exposure, they have had significant repercussions for atomic veterans and their families. The true health, psycho-social, and cultural costs of the tests are only beginning to emerge. The chapter concludes with a table of statistics that describes the outcomes for these veterans internationally.
Nuclear weapons testing was undertaken on a few remaining colonies. They were isolated, far from home, out of sight and out of mind, except when successful tests were reported to the media with pride and bombast. Island and desert outposts were used, far away from “civilised” humanity, and barely registering on the map to most people. The colonial geographies of the nuclear weapons tests were reported as uninhabitable wilderness by the senior military officers who chose them. This was often far from the truth. Local communities were forced from their homes and sacred lands at best; or they were left there to become human guinea pigs at worst, potentially exposed to high doses of ionising radiation (Thakur, 1996).
The men who tested the nuclear weapons were from the countries that later became the five nuclear weapon possessor states: the USSR, UK, US, France and China. These men were often young and uneducated, with little information about the risks they could face (Alexis-Martin, 2016). Many of them were undertaking their national service, or a similar conscription programme. In an era when travel was very expensive for the average person, testing nuclear weapons offered them opportunities to see the world. They travelled away from the tightly-knit social regulation of family and life-long friends, away from everything familiar, and were jumbled up into regiments with a random assortment of other soldiers. This was the first time that many of these men would be able to define themselves on their own terms. There are issues of medical, social, cultural and environmental justice surrounding their experiences. Some men were also involved in the remediation of these atomic places, attempting to restore the original geography and ecology, and to try and remove traces of this nuclear attack to the land (Pyne, 1995).
In common with other members of the military community, the nuclear test veterans experienced adverse conditions during their work. Although they were not under enemy fire or placed directly within any conflict zone at the time of testing, these men were involved in the development of the most powerful and deadly weapons known to humankind. The demographic was skewed to begin with, as many were very young and from lower socioeconomic groups, or were conscripted for services during the aftermath of WWII. These men returned home from testing and began their lives, meeting partners and having children.
In the early 1980s, media interest highlighted concern among veteran’s organisations that British nuclear test participants could be subject to ill health (Muirhead et al. 2003). An interest in the potential effects of nuclear weapons testing has since resurfaced in the 2000’s, due to the advent of affordable genetic testing, and a greater prominence of issues such as hereditary health effects, genetic diseases and chromosomal aberrations within the media (Rowland et al 2007; Wahab et al 2008). This has reinvigorated concerns, with a focus upon the wellbeing and health of the descendants of the nuclear test veterans. Veterans perceive that they have not been treated satisfactorily by the MOD, that there is a lack of recognition of their contributions to UK defence, “blocking of access” to information about the tests, and excuses for their treatment by the state (Miles and Green, 2011; The Mirror, 2018).
-
Health and wellbeing
There is considerable contestation and distrust of medicine, the scientific community, and the MOD by the nuclear test veteran community. Academic epidemiological studies to date have been inconclusive (Rabbitt-Roff, 2002), although the National Radiation Protection Board (NRPB) has concluded that mortality and cancer incidence in UK nuclear weapons participants have continued to be similar to those in a matched control group and overall mortality has been shown to be lower than expected from national rates, with no evidence of increased risk of multiple myeloma among test participants in recent years (Muirhead et al. 2003). This could be attributed to the “healthy soldier effect”, whereby the original baseline for military entry-level occupational health is greater than for other professions. This is then sustained by engagement in physical activity, frequent health screening, and significantly better access to healthcare, both during and after military service (McLaughlin et al., 2008; Waller and McGuire, 2011). The healthy soldier effect continues to influence the outcomes of soldiers for up to 30 years (Waller and McGuire, 2011). This is paradoxical scenario, as while their lifestyle may have had a protective effect to the British nuclear test veterans, it may also mask health challenges when compared to populations without the healthy soldier effect.
MOD and independent epidemiological studies suggest that there are no nuclear-weapon related health effects to nuclear test veterans. However, sociological and anthropological research suggests that that that the veterans have notable nuclear weapon related, although not necessarily ionising radiation-linked, health challenges; and that this community attribute their poor health to their time spent testing nuclear weapons (Trundle, 2011). It is notable that there are a range of wider external influences that have contributed to the beliefs of the nuclear test veterans that there is a link between their ill health and test participation, including the comments of health professionals when asked about a link between illness and radiation; media reporting of a supposed causal link; and the views and opinions of other individuals or groups, such as the BNTVA, as significant contributing factors (Miles and Green, 2011). The purpose of this study is not to come to any conclusions about whether the tests have had any direct or indirect impacts upon cohort health, but to understand the experiences and challenges of seeking formal healthcare within the nuclear test veteran family community.
It has previously been reported by a quantitative study that most respondents were very pleased with the services that they had received, with all service types rated ‘good’ or ‘very good’ by over 78% of respondents (Miles and Green, 2011). However, the descendants’ experiences of healthcare have not previously been explored, and UK healthcare has been subject to a number of significant structural and cultural changes since the time of this previous study.
It is challenging to discern the complete health, wellbeing, cultural and social implications of British nuclear weapons testing to veterans and their families. In part, this is because it is difficult to obtain data from all affected regions and nuclear weapons testing participant nations because the topic is still treated with high levels of security and confidentiality. There remains a geography of secrecy. However, studies have been undertaken that try to provide insights into the life outcomes of the atomic veterans.
There are also many challenges with research of this nature that link back to the culture of secrecy that surrounded the weapons tests. Some veterans can be reluctant to talk about their experience or to attribute blame for their health challenges to their state military organisation, due to concerns about prosecution. Other atomic veterans are convinced that the bomb is responsible for their life challenges, resulting in conspiracy theories emerging around their experiences. A singular universal challenge for these communities is in addressing the lack of information that has been provided to them about their experiences and the risks that they and their families may, or may not, face. This information inequality and lack of support has resulted in elevated perceptions of the risk from ionising radiation exposure, within the nuclear community of atomic veterans and their families. This has had repercussions, as perceptions of risk can change life choices.
Very little work had recently been undertaken on the experiences of nuclear veteran families, with a single study of seven atomic veterans and their families in the USA by Murphy and colleagues, published in 1990. This study noted a significant psychological effect to family members. The reasons given for these effects included the invalidation of their experience by government and authority figures, concerns about genetic effects to future generations, a desire to protect each other from fears of physical consequences, and a need to leave a record of their experiences to prevent future suffering.
The US and UK atomic veteran communities, as well as military data pertaining to the tests, have been explored by the scientific, military, and academic communities. There are parallels to the experiences of these transatlantic atomic communities, and therefore parallels to health and lived experiences. Experimental, epidemiological, and cancer studies have provided some evidence of health risks, albeit with uncertainties surrounding radiation doses of 100mSv or less. However, it is very difficult to untangle and identify a single cause for the health challenges that have been experienced by the atomic veterans. There is neither reliable exposure data, nor an understanding of what else they may have been exposed to (DDT, asbestos, beryllium, and other carcinogens were common at the time). Therefore, any evidence of health problems cannot be attributed conclusively to ionising radiation.
The issue of identifying health consequences is confounded by the life choices that atomic veterans make. Being a member of the military has a protective effect to health, known as the healthy soldier effect. Members of the military must go through training, where less healthy individuals leave, creating an elite of healthy people. They led active lifestyles with healthy food during their working years and, as soldiers, they would have received more medical attention and physical inspection than the average population. Most become used to routine medical examination, which can persist after leaving the military. This effect confers a 10-25% decrease in risk of mortality for those who have served in the military, compared to the general population. However, the healthy soldier effect predominantly refers to physical health and wellbeing, with mental health comparatively neglected. For instance, suicides and homelessness are both notable veteran mortality risks.
Academics have undertaken several studies on the US, New Zealand and UK atomic veteran cohorts to try and understand health effects and risk of health problems. Bross and Brosses reanalysis of the 1985 US National Research Council report on Mortality of Nuclear Weapons Test Participants, shows 62% higher incidence of digestive, respiratory, leukaemia, and other cancers among soldiers involved in nuclear weapons testing whose reported doses were over 300 mrem.
In the UK, there have been several epidemiological studies of British nuclear test veterans, including three studies by Darby and Muirhead in the 1990s. However, difficulty arises again due to confounding factors, as any mortality or cancer incidence detected may be due to other agents or exposures. It’s known that ionising radiation was not the only risk, and that the healthy soldier effect goes some way to offer a protective capacity, so it is very difficult to tease out the true impact of ionising radiation. Muirhead and colleagues published a study in 2003 that explored the health effects to a total of 21,357 servicemen and civilians who participated in the tests and were followed over 1952-1998. This group was countered by a control group of 22,333 men who had not participated in nuclear weapons testing. Analyses were conducted for mortality and incidence for 27 types of cancer. It’s important to note that this study showed that overall mortality and cancer incidence in UK nuclear weapons test participants have remained similar to those in the control group, who have no suspected exposure to ionising radiation.
Overall mortality remained lower than expected, compared to national rates. This study showed that there was no risk of multiple myeloma risk among participants. However, there was some evidence of raised risk of leukaemia among test participants, relative to controls, particularly in the years immediately after nuclear weapons testing. However, this could be a chance finding, due to unexpectedly low rates among the control group and the generally small radiation doses recorded for test participants – nonetheless, the possibility that test participation caused a small increase in absolute risk of leukaemia cannot be ruled out. A further study by Muirhead et al in 2004 demonstrated that there was no evidence of increased risk of multiple myeloma among test veterans in recent years.
In the late 1990s, Roff et al surveyed the members of the British Nuclear Test Veteran’s Association (BNTVA) to try to identify health problems, but there are a number of issues with her work. Whilst it provides a good broad insight into the challenges that are faced by this community, their health problems are self-reported and, because they are all BNTVA members, they are more likely to attribute these problems to ionising radiation. Her statistical study of 1041 members showed that 84% reported health challenges, included skin conditions, dental problems, a small percentage of participants experiencing cataracts before the age of 40, infertility, early hearing loss, and early heavy hair loss. Health issues were also reported among 39% of children and 21% of grandchildren. Unfortunately, there is a need for medical records to back up this study, and the self-selected nature of the approach means that those who have experienced difficulties with health are more likely to come forward.
A study of Australian veterans of the British nuclear tests showed that all-cause mortality was not elevated (Gun et al, 2008). However, mortality and incidence were raised for cancers of the head and neck, lung, colon, rectum and prostate, and for all cancers combined. For oesophageal cancer, melanoma and leukaemia, incidence was significantly raised but mortality was not significantly raised. Again, our ‘healthy soldiers’ may have experienced more medical check-ups that meant that their health challenges were managed more effectively. It is worth noting that melanoma is associated with sun damage, which may offer a more plausible explanation for skin cancers among the predominantly Caucasian soldiers working in the Australian desert. Oesophageal cancer is also common among those who drink alcohol and smoke heavily, two lifestyle factors of the era, especially in the military. This study found that there was no association between radiation exposure and overall cancer incidence or mortality, or of any cancer or cancer deaths occurring in excess. Contributing factors included smoking, alcohol and asbestos exposure, and demographic differences to the Australian population with whom the veterans were compared.
More recent studies in the USA have shown that exposure to low-dose ionising radiation does cause a tiny increase in the risk of leukaemia, although it’s debatable as to whether this risk is significant. There is clearly further work needed to understand the issue of health and the atomic veterans. The Million Persons study is currently attempting to resolve some of the lingering questions that remain, including 115,000 atomic veterans in its cohort of people who may have had an occupational radiation exposure. Veterans have been traced through military records to remove the effects of self-selection. The study is trying to discern the risk from gradual exposures over time, rather than brief exposures to elevated doses of ionising radiation. It explores the consequences of internal and external doses of ionising radiation. Its aim is also to estimate the lifetime risk of radiation-induced leukaemia. Perhaps this study will provide some more concrete answers about experiences of health within the veteran community.
Just because you cannot see a problem, doesn’t mean that it isn’t there. Health challenges attributed to environmental exposure are frequently contested. Diagnosis is complex, and our scientific understanding is limited. Sometimes conditions can be unaccepted by the medical community, or unmedicalised until it is accepted that there is a problem. Examples of conditions that have historically been unmedicalised include chronic fatigue syndrome, post-traumatic stress disorder, and Gulf War syndrome. However, there are specific difficulties with gaining recognition of an environmental exposure.
Trundle’s work has explored the experiences of the nuclear test veterans and determined that they needed to provide three levels of “proof” to gain state recognition for their illnesses: a biomedical disease label from sanctioned medical experts, proof of exposure, and proof of a causal link between exposure and disease. For many nuclear test veterans this is impossible. Illnesses often remain unmedicalised or invisible, there is a lack of records of individual exposure rates, and it is very difficult to prove a link in the form of a scientifically legitimised and politically recognised aetiology. Among nuclear veteran communities, a diagnostic practice is desired that affirms the somatic nature of illness, but also asserts a politically and morally configured notion of culpability.
Atomic veterans often want a medically verified explanation for their illnesses, and actively work to try and remove perceived negative political influences from the diagnostic process. This means that they contest some explanations of their diagnoses, for example ascribing their skin cancer to ionising radiation as well as, or instead of, solar radiation. Whilst not denying the biological nature of their afflictions, the atomic veterans place a significant emphasis upon revealing a political cause for their disease – i.e. Government culpability. This can be described as a quest for a biopolitical endpoint, where historical narratives are included about a nation’s shame and a state’s admission of guilt. The veterans are demanding an endpoint that enables them to assume the status of a collective who have endured a grave injustice and are therefore perceived to be entitled to public recognition, state resources, a service medal and an apology. However, it has been extensively debated as to whether medals should be awarded.
Internationally, atomic veterans claim to suffer multiple health problems from radiation exposure and seek compensation from state. They contest and devalue military and medical records, and instead they elevate their personal and collective memories, based on what they have witnessed. An example of this is the myth of the “x-ray hands”, where veterans of Christmas Island claim that they saw through their gloves and skin, right through to the bone, due to ionising radiation during the nuclear weapons tests. However, the type and nature of ionising radiation produced during the blasts would not enable such a phenomenon. A more likely explanation is the powerful burst of light produced at the moment of detonation.
Atomic veterans’ organisations continue to resist state evidential and archival materials. They accept certain documents as historical truths, but only if they confirm the communities’ understanding of the atomic scenario and emerge from archives without state sanction. Atomic veterans’ organisations have therefore created their own private archives, which function as sites of legitimisation for their perspectives, perceived legal proof, and serve to memorialise other members of their community. Therefore, the atomic veterans’ organisations subvert and mimic the documentary logic that already exists within state records. They are reluctant to share their archives with other organisations, which makes it difficult to gain a true understanding of their experiences and perspectives.
There is considerable support available for atomic veteran communities internationally, and specific schemes have been implemented by USA, French, Australian, New Zealand, Fijian and British governments. Still, these communities campaign for more support. They desire more funding to try and understand their own experiences, and to try to ensure that their descendants receive ongoing support for their reported health challenges.
In the UK, British nuclear test veterans are supported by a MOD team that addresses their specific health concerns and helps with their applications to the Armed Forces Compensation Scheme. In addition to this, further support is provided for initiatives such as Armed Forces Day and for HM Armed Forces veteran’s badges. Support has also recently been provided in the form of large-scale government funding for independent research.
Since 2012 a majority of veterans have campaigned for both Government recognition and National recognition by way of a medal. Government recognition was achieved on 2nd July 2014 in a statement by the then Prime minister David Cameron at the dispatch box, however, the campaign for medallic recognition by the Nation continues. An unofficial paramilitary medal that was commissioned by the British and Australian nuclear test veteran’s associations can be purchased for £45 online, and many veterans own this medal. The UK has one major support and issue campaign group for this: the British Nuclear Test Veterans Association (BNTVA).
In the USA, compensation is available to veterans who have any one of 21 cancers that are traceable to radiation exposure – these men are entitled to a one-time award of up to $75,000 or a monthly disability payment from the Department of Veteran Affairs. However, there are concerns about access to this scheme – it is difficult to verify records of service, and there is no formal discharge form for US atomic veterans. There are also difficulties surrounding the culture of secrecy around US nuclear defence work, which meant that veterans could not discuss their experiences until 1996. However, whilst the DD-214 discharge form does not mention atomic weapons testing, it is widely known that this signifies work undertaken on atomic weapons. Just like in the UK, those involved in clean-up operations, such as the Enewetak Radiological Clean-up, are in a place of limbo as they have not been formally recognised as atomic veterans in the same way as those men who directly participated in weapons testing, despite having participated in a radiation risk activity.
American veterans are also supported by the National Association of Atomic Veterans (NAAV), an organisation that provides solidarity and pursues their cause, formed by a group of ex-military personnel who were first-hand participants in the US atomic testing program. NAAV has successfully campaigned for a US Government Radiation Dose Reconstruction team to approximate radiation exposure to atomic veterans, as part of the Million Person Project. The NAAV has suggested that they want the government to acknowledge that this community were subjected to an unusual risk, beyond usual military service. They also feel that the government should provide them with appropriate medical care for conditions that may be due to exposure to ionising radiation. Similarly to the UK, some in the community feel that they should receive financial compensation for their work, whereas others want no more than official recognition by way of a certificate or medal.
-
Hidden Communities
Internationally, there is a hidden community who have been affected by the nuclear tests, and who are not always supported: the wives and children of atomic veterans. This community often feel at risk from the ionizing radiation their family members may have encountered. This community also experiences the hidden challenges of caring for and supporting aged veterans. There is a great concern within atomic veteran communities that their roles in the atomic bomb will have genetic effects, adversely impacting their children. However, any spermatozoa affected by the radiation will have been naturally replenished before they could cause any genetic defects, so long-term genetic health effects are extremely unlikely. However, the concern and anxiety caused by this perception of risk is undeniable. Moreover, the paucity of information provided to these communities has resulted in an amplified perception of these risks. Some daughters of atomic veterans have decided not to have children due to perceived concerns about damage to their own DNA.
Many of the concerns stem from events that are harrowing, but also common to the normal population. A US study exploring reproductive outcomes for veterans showed that adverse reproductive outcomes are not as rare in the general population as one might think. This includes the inability to conceive, the premature spontaneous termination of a pregnancy, the birth of infants with a congenital malformation, and premature death. The study estimated that 15,000 children with major birth defects would be expected among the 500,000 or so offspring of the 210,000 Atomic Veterans, even in the absence of any radiation effects. This is important, as it quantifies the actuality against the perceived risk, and demonstrates that the community is within the bounds of normality in this sense. It suggests that there is a “atomic veteran’s syndrome” that represents this pattern of health challenges, rather than individual sets of illness.
Historic self-reported health studies showed that one in seven of British atomic veterans in a sample of 1014 did not father any children after they returned from testing, equivalent to 14%. This is also the average rate of infertility for men and women, and the likelihood of male infertility increases with age. There are also other host and environmental factors that influence descendant health outcomes, including maternally or paternally derived inherited defects, exposure to smoking and the consumption of alcohol during gestation, pre-existing maternal illnesses such as diabetes or other illnesses during pregnancy, and poor nutrition. During the 1950s, 1960s and 1970s, these factors would have been more prevalent, as public health measures such as five-a-day for diet and anti-smoking bans were yet to come into place. It is therefore almost impossible to have an epidemiologically valid study of descendant effects and health outcomes, within the domain of low-level ionising radiation exposure.
A study also reported that nearly half of the health problems among the 5000 studied offspring of the nuclear weapons test veterans consist of the same dermatological, musculoskeletal and gastrointestinal conditions that their fathers have also suffered from (Roff, 1999). This is may to be an inherent hereditary, rather than ionising radiation exposure related link, as many of the conditions reported in this study are common hereditary complaints, like eczema, dermatitis and rheumatoid arthritis. Although this provides interesting insights into the experiences of health within the cohort, the reported rates of descendant health conditions are not significantly different to those reported by the general population.
It can be difficult to communicate the reality about the health risks to veterans and their families. Experts and the state may be distrusted, and the veteran communities tend to understand their perception of risk through personal, relational and affective experiences. Risk likelihood among the community is identified based on the misfortune of those that they know, rather than on statistical datasets. This is because data is not easily available in an accessible format, and it does not provide a reflection of the lived experiences of this community. Understandably, the negative experiences of other veterans can capture experiential knowledge, and reveal personal and familial suffering in accessible and relatable ways. Expert evidence from specialists in radiation protection or biomedicine has not convinced this community, because it arises from contested sources. The atomic veterans use their experiences to build narratives about heritable and ionising radiation related illnesses. This has led to high levels of anxiety around health and the influence of genetic heritage.
It is evident from this literature review that there are considerable contestations and clarifications surrounding the nuclear test veteran community, and that research was needed to support their understanding of their experiences, health and wellbeing. The purpose of this report is to develop a better understanding of how health and wellbeing intersect with the lived experiences of nuclear test veteran families, with focus on descendants.
-
Research methodology
The purpose of this project was to collect a diverse selection of qualitative and descriptive quantitative data to provide insights into the lives of the British atomic veterans and their families. Qualitative questions address the purpose, context and meaning of their experiences. This study recruited a cohort of nuclear test veteran families and undertook phased research across the community. Topics that were explored included: wellbeing, mental health, physical health, perceptions of risk, hidden care, and memorialisation and death. The qualitative methodology for this study included questionnaires, semi-structured interviews and oral histories, workshops, and participant observation. It also included the collection and analysis of secondary data, including academic literature, veteran biographies, material from the National Archives, and artefacts from personal collections.
-
Cohort recruitment and study overview
For the purpose of this study, a nuclear veteran family member is defined as someone who has a direct nuclear test veteran lineage or affiliation. This includes all wives, spouses and any other partners of nuclear tests veterans, should multiple partnerships have occurred; all nuclear test veteran children, including sons and daughters; and all grandchildren; including grandsons and granddaughters. The focus of the descendant aspect of the study is on those family members who provide a direct bloodline from the nuclear test veteran. However, a number of step-children and adopted children were also interviewed, to explore any differences of experience between the two groups (i.e. differences in perception of risk or childhood experience).
The majority of the cohort were formally or informally affiliated with the Old BNTVA, Fission Line, or Fallout, an online group for nuclear test veteran descendants. As these groups campaign to raise awareness and for financial compensation for perceived damage to test veteran health, it was anticipated the cohort would believe that there was a link between their participant in the tests and their or their families’ poor health. The cohort was accessible and there were no challenges of communication or recruitment. Individuals self-selected and volunteered to participate in our research after the study was advertised online within relevant social media groups and within the BNTVA Campaign quarterly magazine. A snowball sampling approach was taken to encourage individuals to recruit their family members to the study, creating family sets. This allowed for interfamily and intergenerational differences in attitude to be explored.
Cohort recruitment continued for approximately the first eighteen months of the study, from June 2016 to January 2018. During this time, 500 respondents were contacted in total. Fig 1 shows that, of the 500 responses that were elicited by the Nuclear Families study, 300 respondents provided an initial response to the study call, 230 participants provided a questionnaire reply, 112 participants provided a short interview, 78 participants provided an in-depth interview, and 25 participants were included in a wellbeing or memorialisation ethnography.
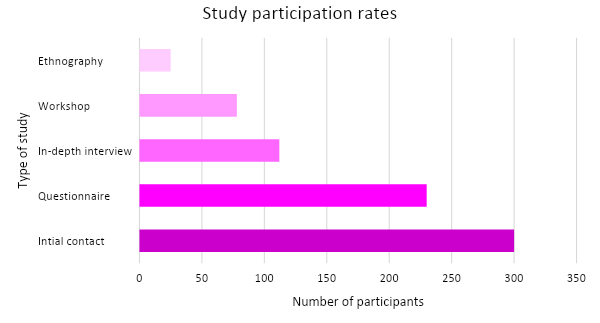
Fig 1. Participant response rate to a) initial contact, b) questionnaire, c) short interview, d) in-depth interview, e) wellbeing or memorialisation ethnography.
This represents an expected dynamic across the lifespan of the study, as ethnographic research requires a significant long-term commitment from both the participant and researcher, but generates a large amount of useful qualitative data. These methods were selected to provide a diverse array of data that provides individual and collective perspectives and experiences of being part of a nuclear test veteran family.
The questionnaire provided a fixed script of basic demographic, wellbeing, attitude and opinion questions with closed answers that can be administered in person, online, or over the phone. The semi-structured interviews and oral histories, where relevant, were conducted one-on-one between an interviewer and individual, to collect information in a less structured way that enabled the interviewee to share their experiences and understanding of relevant topics. Interviews took place in person, over the phone and via Skype. Focus groups provided dynamic group discussions and were used to understand collective opinions and experiences, and to help community members to share their understandings through interaction. Ethnographic studies provided overt observation of nuclear test veteran family and community members, without direct researcher participation. This approach provides insights into lived experiences of participants over a longer timescale, by exploring interactions and processes surrounding nuclear test veteran family life. Data collection was complemented by personal, archival and academic secondary data resources. Data has been selected and combined across datasets, to provide the most compelling insight into nuclear test veteran family life.
Table 1. The benefits of focus groups vs. interviews vs. questionnaires (adapted from Harrell and Bradley, 2009).
|
|
Focus Group |
Interview |
Questionnaire |
|
Depth of information |
x |
x |
|
|
Resolve conflicting information |
x |
x |
|
|
Relative emphasis on value |
|
x |
x |
|
Generalisability |
|
x |
x |
|
Avoid “participant fatigue” |
x |
x |
|
|
Topic sensitivity |
|
x |
x |
|
Topic classification |
|
x |
x |
Table 1 highlights some of the positive and negative aspects of the different methodologies that were used in this study. This combined approach offered insights into how behaviours and relationships change and/or are maintained among the nuclear test veteran community and provided a “normal context” for participants’ behaviours, interactions and opinions. Ethnographic work was undertaken at BNTVA[2] events and memorialisation ceremonies, to better understand the intergenerational interactions of the community. Workshops and workgroups were provided at the University of Southampton and at BNTVA events. These workshops provided a safe space for the British atomic veteran community to discuss and explore their experiences. The participant-led workshops were supported by atomic veteran daughter Susan Musselwhite, and enabled Nuclear Families research across topics to be targeted and explored. This combination of approaches provided opportunities for a variety of different demographic groups within the nuclear test veteran community to participate, but also provided different ways to gain insights into nuclear test veteran family life.
-
Semi-structured interview and questionnaire
Semi-structured interviews provide an interviewer-guided discussion about particular themes or topics that are relevant to the study. The semi-structured interview guide provides a clear set of instructions for interviewers and can provide reliable, comparable qualitative data. Semi-structured interviews are often preceded by observation, informal and unstructured interviewing in order to allow the researchers to develop a keen understanding of the topic of interest necessary for developing relevant and meaningful semi-structured questions. The inclusion of open-ended questions and training of interviewers to follow relevant topics that may stray from the interview guide does, however, still provide the opportunity for identifying new ways of seeing and understanding the topic at hand (Bauman and Greenberg, 1992).
Semi-structured interviews are a flexible and powerful tool to understand, interrogate and corroborate different individuals’ perspectives, in this case, their experiences of being a nuclear test veteran or family member. This process includes six stages: (a) selecting the type of interview; (b) establishing ethical guidelines, (c) crafting the interview protocol; (d) conducting and recording the interview; (e) crafting the interview analysis; and (f) reporting the findings (Raboniet, 2011).
Typically, the interviewer has a paper-based interview guide that he or she follows. Since semi-structured interviews often contain open-ended questions and discussions may diverge from the interview guide, it is generally best to tape-record interviews and later transcribe these tapes for analysis. Participant consent was gained for all recordings undertaken for this aspect of research. The questions included in the semi-structured interview explored a variety of topics, from demographic and contextual queries, to questions about perception of risk from hereditary and genetic effects of ionising radiation.
Some informal interview observations were also undertaken as part of this study, where informal interviews are casual conversations one might have with the people the researcher is observing, without a structural guide.
-
Focus group methods
Participant focus groups are a way to understand the perspectives of specific demographics in the study, and to provide a safe and guided environment to explore and compare their experiences. They are a popular method in human geography, as they generate rich conversational data that provides insights into complex social issues (Crang, 2002; Flowerdew and Martin, 2005). The basic format of a focus group is ‘a group of individuals selected and assembled by researchers to discuss and comment on, from personal experience, the topic that is the subject of research’ (Powell et al, 1996: 499). In terms of group size, each focus group discussion should include between four to ten participants as an ideal, with a researcher and facilitator or support academic, to help to facilitate and moderate their conversation. After an introduction, the focus group proceeds as an issue-based discussion, with participants contributions in the ways and at the times that they wish to (Flowerdew and Martin, 2005). The text is supplemented by moderators notes that explore aspects such as group dynamic, mood, interactions and similar, to produce a rich qualitative insight into the focus group conversation. This method is useful, as it gives insights into the spectrum of views that individuals hold regarding a particular issues; and the nature of their interaction and dialogue over time. In the context of this study, focus groups were delivered and prepared to explore:
- Interactions and experiences of nuclear test veteran fathers and sons.
- The experiences of nuclear test veteran descendant mothers and daughters.
- The experiences of nuclear test veteran descendant fathers and sons.
The Nuclear Families focus group sizes ranged from six to ten participating individuals per focus group. Participation was voluntary and stand-alone, with some participants who were included across other study areas, but others who solely contributed to the focus group.
-
Participant observation methods
Participant observation and ethnographic methods were used to explore the day-to-day and event lives of nuclear test veterans and their families. Non-participant ethnographic research is done from a distance, in order to not influence the behaviour of the participant, whereas participant observation allows interaction with participants in order to understand daily rituals and behaviours (Gobo, 2008). Furthermore, participant observation involves a distinct interest in human meaning and interaction, and the perspectives of others (Jorgensen, 1989). Ethnographers generate understandings of culture through representation of what we call an emic perspective, or what might be described as the “‘insider’s point of view.” The emphasis in this representation is on allowing critical categories and meanings to emerge from the ethnographic encounter rather than imposing these from existing models. An etic perspective, by contrast, refers to a more distant, analytical orientation to experience (Hoey, 2014). Researchers also collect other sources of data which depend on the specific nature of the field setting, this may take the form of representative artefacts that embody characteristics of the topic of interest, such as government reports, newspaper and magazine articles (Hoey, 2014).
This makes observational approaches useful for studying community interactions, family dynamics and the general wellbeing of nuclear test veteran families. In the context of the study, overt participant observation was undertaken during a series of nuclear test veteran memorialisation events and Nuclear Families workshops from 2016 to 2018. Individual family ethnographies were also undertaken with members of the community who were gauged to have experienced intergenerational challenges relating to health and wellbeing, as determined by the questionnaire. Research participants were provided with study purpose guidelines, and were required to complete participant consent forms as part of the research process. Photography, audio-recordings and field notes were used to document their experiences and artefacts related to nuclear weapon testing, and to record perceptions, interactions and conversations that occurred during ethnographic work. A wealth of material emerged from this process, as study participants shared their nuclear test veteran family members’ personal archival material and memorabilia relating to their time in service.
-
Ethical Protocol
This study gained ethical approval from the University of Southampton (Approval: 19266). The process required the successful completion of ETHOS risk assessment and ethical protocol documentation, which was presented to an ethical review board at the University of Southampton for approval. Sample ethical documentation is provided in Fig 2.Further details of the ethical review process are available from the University of Southampton and included in the Appendices of this study. No one under the age 18, no one with severe degenerative memory loss, and no adults with severe learning disabilities were included in this study. To ensure consenting study participation, participants were provided with a copy of a research purpose statement, a participant consent form, and were given further support organisations to contact should any challenges arise following study participation. Participation in the study was not compulsory and participants were made aware of their right to withdraw from participant, or to withdraw their data from the study at any time, and provided with contact details to do so if necessary. All study participants were invited to remain in contact with the project throughout the Nuclear Families research process by receiving email updates. All data has been retained on an encrypted password-protected computer. All identifying features have been removed to protect the identities of study participants, unless they have specifically chosen to be included in this report and further publications, non-anonymised and ad-verbatim. One study participant wholly withdrew from the study during its duration, and their details have been removed from all datasets and data presentations, in reports or otherwise.
Research Title:

Principal Investigator:


Research Funder (if applicable):
|
|
YES |
NO |
|
X |
|
|
|
X |
|
|
X |
|
X |
|
|
|
X |
|
X |
|
|
X |
|
|
|
X |
|
|
X |
|
|
X |
|
|
X |
|
|
X |
|
|
X |
|
X |
|
|
X |
|
|
|
X |
Fig 2. Ethical Approval Checklist, University of Southampton, 2016.
-
Questionnaire Outcomes
Questionnaire results were elicited throughout the study. The questionnaire was provided to 500 respondents in total, of which 230 individuals provided a response. The questionnaire was delivered in a number of ways; including in-person at nuclear test veteran events, project workshops, as part of the semi-structured interview process; at the homes of in-depth interview respondents, as part of the semi-structured interview process; on Skype, as part of the semi-structured interview process; though the post with a stamped and addressed return envelope to those recruited during the study sign-up process; by telephone interview, and by email mail-out to study respondents. The high response rate reflects this multifaceted strategy. Fig 3 shows the proportion of responses elicited according to the mode of questionnaire receipt.

Fig 3. Proportion of questionnaire respondents by response mode, n = 230.
It is notable that the most successful data collection strategies were in person. It should also be noted that one participant withdrew their response at a later date, leaving 229 questionnaire responses in total.
This section presents results and provides an analysis of quantitative data collected through the questionnaire. The questionnaire design and method can be viewed in Section 1.4.2. and Appendix 7. These results provide insights into the overarching study demographic and their experiences of being part of a test veteran family. The results explore gender, age, marital status, participant health behaviours and perceptions of risk.
-
Gender
 Fig 4. Gender of questionnaire respondents, n = 229.
Fig 4. Gender of questionnaire respondents, n = 229.
Fig 4 provides insights into the gender of questionnaire respondents. The questionnaire elicited more female participants than male, including several more daughters than sons. This may reflect challenges in retaining and maintaining male study participation compared to the female cohort. It may also be that female participants may be more willing to provide information to a study of this nature, than male participants (Patel, et al. 2003). More female participants also participated in other aspects of the study, including interview and ethnographic work.
-
Age
Fig 5 provides insights into the age range of respondents. Participants were recruited across the adult age demographic. Children under the age of 18 were excluded from this study for ethical reasons. Those under the age of 25 represented a minority of questionnaire respondents, with eight responses elicited. This is likely to be because younger respondents are grandchildren, and may be less aware of their nuclear test veteran family heritage. Alternately, grandchildren may have been travelling, studying, or otherwise spatially unavailable during the time the the study. Over half of the study (155 respondents) were aged between 36 and 65. This proportion represents the nuclear test veteran direct descendant community, as expected. However, a larger proportion of respondents than expected were aged 66+ (68 respondents). This included responses from nuclear test veterans and their current and previous wives, partners and spouses. This willingness to participate could have been for a variety of reasons, including concerns about the wellbeing of descendants, or having more time to talk in retirement (Mody et. al. 2008).

Fig 5. Age of questionnaire respondents, n = 229.
-
Marital status
This section of the questionnaire asked respondents about their previous and current relationship status, marking relationship milestones. More nuclear test veterans had been married, divorced, separated or widowed than their descendants. This reflects the family and descendant-oriented nature of the study. Occurrence of divorce per veteran is more abundant than expected. Section 3.3 considers some of the reasons for this, through interview data about mental health and military relationship cultures (Dermott and Gatrell, 2018). Fig 6 provides insights into nuclear test veteran relationships. It is notable that some nuclear test veteran respondents selected multiple scenarios, as they had experienced several different relationship phases throughout their lives. Overall, there are intergenerational differences, with a greater occurrence of family dynamic change among nuclear test veteran participants than descendants.
 Fig 6. Lifetime marital status of nuclear test veterans (includes multiple historic divorces and marriages) n = 67.
Fig 6. Lifetime marital status of nuclear test veterans (includes multiple historic divorces and marriages) n = 67.
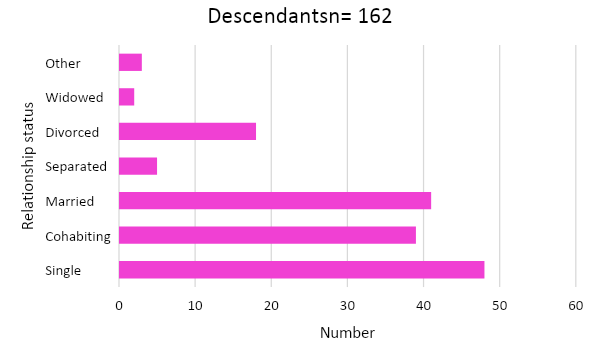 Fig 7. Marital status of nuclear test veteran descendants, n = 162.
Fig 7. Marital status of nuclear test veteran descendants, n = 162.
Fig 7 shows the diversity of relationship types among descendant participants, who are more likely to report cohabitation or single status than nuclear test veterans, but less likely to be widowed, married or divorced. While veterans did not provide ‘other’ relationship scenarios, for descendants, some more unusual and individual scenarios included intentionally platonic parenting and polyamory.
-
Physical health
This section of the questionnaire explored the physical health of nuclear test veterans and descendants, with focus upon self-reporting of disability and its impacts on daily life. A proportion of nuclear test veteran and descendant respondents reported experiencing physical health challenges. Fig 8 showed the proportion of this community who experience difficulties, compared to those who attribute their physical health to challenges to their capacity to undertake work and socialise. While veteran’s reported incidence of physical disability (46%) is in line with 45% expected for those of pension age, it is notable that the proportion of descendants of working-age who self-report living with physical disability (28%) is considerably higher than the expected 19% disability incidence for working-age people (Scope, 2018).
 Fig 8. The proportion of a) nuclear test veterans, and b) descendants, who consider themselves to have a physical disability, and who report that their disability has affected their capacity to work (%), compared with UK national average (%) disability incidence (Scope, 2018).
Fig 8. The proportion of a) nuclear test veterans, and b) descendants, who consider themselves to have a physical disability, and who report that their disability has affected their capacity to work (%), compared with UK national average (%) disability incidence (Scope, 2018).
Both respondent demographics who described themselves as physically disabled reported challenges in working and socialising. Veterans were less likely to report these specific challenges (17%), compared to descendants (21%). This may be because veterans are more likely to be retired and therefore less likely to engage in work.
 Fig 9. The proportion of a) nuclear test veterans, and b) descendants, who have a physical disability, and consider their physical disability to be associated with their nuclear test veteran heritage (%).
Fig 9. The proportion of a) nuclear test veterans, and b) descendants, who have a physical disability, and consider their physical disability to be associated with their nuclear test veteran heritage (%).
More descendants (46%) than nuclear test veterans (21%) associated their physical health with their nuclear test veteran heritage. Fig 9 demonstrates how a proportion of members of both the veteran and descendant communities attribute their physical health challenges to their nuclear test veteran heritage, as other adequate explanations may not have been provided. Fig 10 shows that few veterans (4%) or descendants (1%) have reported any preconceptions or stigma as a result of their physical health challenges. The slightly higher figure for veterans could reflect changing attitudes over time, or just a longer lifespan of different experiences. This result is positive, as it shows that while the nuclear test veteran community experience challenges with physical health, they do not feel discriminated against for their disabilities.
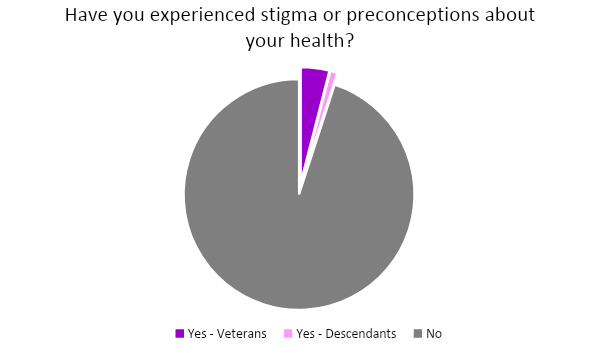 Fig 10. The proportion of a) nuclear test veterans, and b) descendants who have experienced preconceptions or stigma as a result of their physical disability (%).
Fig 10. The proportion of a) nuclear test veterans, and b) descendants who have experienced preconceptions or stigma as a result of their physical disability (%).
More information about physical health is available in Section 3.2. It is notable that some questionnaire respondents who were also interview study participants described symptoms of their physical disabilities, but did not necessary consider themselves to be disabled.
-
Mental health
Both nuclear test veteran and descendant respondents self-reported a variety of mental health challenges. Mental health challenges were also described during interviews, as detailed in Section 3.3. The interview process elicited slightly different results to the questionnaire, whereby veterans described their historic experiences of mental health in their own unmedicalised terms (Bryant et al., 2008). Fig 11 showed that nuclear test veterans and spouses were less likely to describe themselves has experiencing a specific condition, compared to descendants. It also showed that a range of common mental health challenges are self-reported as being experienced by respondents. Descendants were more likely to report experiencing mental health challenges, and to specify their condition(s). Notably, Fig 11 showed higher than anticipated self-reporting of anxiety and depression among the descendant community.
 Fig 11. Proportion of a) Nuclear test veteran, and b) descendant self-reporting of common mental health challenges, including PTSD, anxiety, depression, panic attacks or and/or other mental health symptoms (%).
Fig 11. Proportion of a) Nuclear test veteran, and b) descendant self-reporting of common mental health challenges, including PTSD, anxiety, depression, panic attacks or and/or other mental health symptoms (%).
Fig 12 showed that descendants are more likely to be receiving medical treatment for mental health than nuclear test veterans. This may be due to different intergenerational attitudes towards seeking mental health diagnoses, whereby older adults are less likely to be referred for mental health problems by their GPs, or to disclose mental health challenges to researchers (Mayor, 2017; Olfson et. al. 2002).
 Fig 12. Proportion of a) nuclear test veterans and, b) descendants who self-report receiving treatment for their previously-declared mental health condition(s) (%).
Fig 12. Proportion of a) nuclear test veterans and, b) descendants who self-report receiving treatment for their previously-declared mental health condition(s) (%).
Fig 12 suggests that a notably lower proportion of veterans (4%) and descendants (23%) received treatment, than have a mental health condition overall. This may be due to not all conditions requiring a medical treatment, and also because of veteran reporting of historic instances of mental health. It may also reflect the stigma that can sometimes surround mental health treatments. Fig 13 showed that there was some intergeneration similarity in mental health experiences. However, descendants are more likely to report that another family member experiences similar symptoms, compared to nuclear test veterans. The most frequently self-reported mental health issues for nuclear test veterans were PTSD (19%) and depression (16%); whereas descendants reported experiencing anxiety (31%) and depression (27%) most commonly. Panic attacks and other conditions, explored further in Section 3.6, are both infrequently self-reported by descendants, and rarely reported by nuclear test veterans.
 Fig 13. Proportion of a) nuclear test veterans, and b) descendants who report that family members experience similar mental health symptoms to them (%).
Fig 13. Proportion of a) nuclear test veterans, and b) descendants who report that family members experience similar mental health symptoms to them (%).
A proportion of respondents with mental health challenges said that family members experienced similar symptoms. Descendants were more likely to report that a family member experiences similar challenges (31%). This may reflect the presence of siblings with similar conditions, or greater awareness of family mental health. This is explored further in Section 3.3. To conclude, there is a greater self-reported prevalence of certain mental health challenges within the respondent community.
-
Welfare and wellbeing
There are both veterans and descendants with disabilities, who are in receipt of government financial assistance to help to support their health conditions. Fig 14 provided insights into the proportion of veterans and descendants in reciept of support. Those who do not currently receive benefits, but who reported experiencing physical and/or mental disabilities, were signposted to government, BNTVA and NCCF resources for further support. Fig 15 revealed that some respondents are dissatisfied with the amount of support that they receive. This suggests that goverment support is not always sufficient to provide adequate adjustments for those with disabilities to participate in usual daily life. Participants provided interview responses to this question, that are reviewed in Section 3.2. Some respondents declined to answer questions on government financial assistance.
 Fig 14. Proportion of a) nuclear test veterans and, b) descendants in receipt of government financial assistance to support their health (%).
Fig 14. Proportion of a) nuclear test veterans and, b) descendants in receipt of government financial assistance to support their health (%).
More veterans than descendants reported being in receipt of government financial assistance for their health . This may be due to the increasing incidence of disability with old age (Verbrugge and Yang, 2002). Of those in receipt of government financial assistance to support their health, Fig 15 shows that descendants were more likely than veterans to report that their level of assistance was not sufficient.
 Fig 15. Proportion of a) nuclear test veterans, and b) descendants who describe their financial support assistance to support their health as adequate (%).
Fig 15. Proportion of a) nuclear test veterans, and b) descendants who describe their financial support assistance to support their health as adequate (%).
Fig 16 revealed that there is a differential between nuclear test veterans and spouses, and descendant’s self-ranking of day-to-day wellbeing. Veterans and spouses rated more highly on the Likert scale that was provided in the questionnaire to review and assess their day-to-day quality of life. This may reflect the contemporary experience of retirement age, whereby life satisfaction can increase with time, if relational wellbeing features, such as social networking and financial stability, are high quality (Chei, 2018). Alternately this could be due to percieved social constraints and norms around expressing dissatisfaction. Conversely, descendants ranked themselves as having lesser wellbeing than veterans, an outcome explored in more depth in Section 3.
 Fig 16. a) Nuclear test veteran and spouse, and b) descendant’s proportional response to wellbeing Likert scale (%). Veteran n = 62, Descendant n = 150.
Fig 16. a) Nuclear test veteran and spouse, and b) descendant’s proportional response to wellbeing Likert scale (%). Veteran n = 62, Descendant n = 150.
-
Lifestyle
Lifestyle factors including tobacco and alcohol consumption play an important role in long-term morbidity and mortality, as excess consumption can be life-limiting and affect health (Bien and Burge, 1990). The purpose of this question was to discern respondent self-reporting of health behaviours, with focus on tobacco and alcohol consumption among nuclear test veterans and descendants. Fig 17 shows the proportion of nuclear test veterans (23%) and descendants (18%) who reported tobacco consumption. In 2015, of all adults in the UK, 17.2% smoked, (ONS, 2017). Self-reported tobacco consumption is slightly higher than average for descendants and notably higher for nuclear test veterans. This may be due to increased prevalence and persistence of long-term tobacco consumption among armed forces members and veterans (Hooper et. al. 2008).
 Fig 17. The proportion of a) nuclear test veterans, and b) descendants who report tobacco consumption (%).
Fig 17. The proportion of a) nuclear test veterans, and b) descendants who report tobacco consumption (%).
Fig 18 shows the cigarette consumption habits of respondents who described themselves as smokers. Cigarettes are the most commonly smoked tobacco product, so provide a good gauge for smoking behaviours. The figure shows that descendants who do smoke are more likely to smoke fewer cigarettes per day than nuclear test veterans. This may reflect ongoing overarching demographic trends in smoking reduction and cessation (Edwards, 2018).
 Fig 18. Frequency of tobacco consumption on a daily basis, among a) Nuclear test veterans, and b) descendant smokers (%).
Fig 18. Frequency of tobacco consumption on a daily basis, among a) Nuclear test veterans, and b) descendant smokers (%).
Alcohol consumption was also considered, nuclear test veterans and descendants reported their weekly alcohol consumption, as shown in Fig 19. Responses ranged from teetotal to the consumption of 16+ units peer week; where one unit is equivalent to one spirit measure, ½ pint of beer or lager or a small glass of wine.
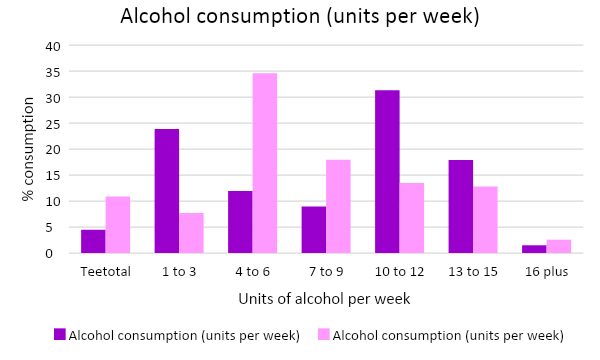 Fig 19. The proportion of a) nuclear test veterans, and b) descendants who reported their frequency of alcohol consumption on a weekly basis, among a) nuclear test veterans (n = 156), and b) descendants (n = 67) (%).
Fig 19. The proportion of a) nuclear test veterans, and b) descendants who reported their frequency of alcohol consumption on a weekly basis, among a) nuclear test veterans (n = 156), and b) descendants (n = 67) (%).
Fig 19 shows that descendants reported an overall lower weekly alcohol consumption than nuclear test veterans, with a preference for 4 to 6 units per week. Veterans were more likely to consume alcohol more frequently, and less likely to be teetotal than descendants. High alcohol consumption (16 units plus) was low in both groups). These lifestyle factor questions support the information provided in health and wellbeing interviews described in Section 3.
-
Caring and care
Care responsibilities are abundant across the nuclear test veteran community, and this is evidenced by the response to this section of the questionnaire. Care responsibilities are intergenerational, and arise for a variety of reasons that are explored further in Section 5.
 Fig 20. The proportion of a) nuclear test veterans and spouses, and b) descendants who report having care responsibilities.
Fig 20. The proportion of a) nuclear test veterans and spouses, and b) descendants who report having care responsibilities.
It is notable that a larger proportion of descendants (32%) experience caring responsibilities, compared to veterans (21%). This may relate to intergenerational care undertaken by descendants, representing a combination of childcare and support of aged parents. Veteran care may relate to spousal support and care of children and grandchildren. More information about the nature of care undertaken by respondents is detailed in Section 6.
-
Hereditary concerns
This section identifies the prevalence of hereditary concerns, with focus on those in the nuclear test veteran family community who may have an elevated perception of risk of their likelihood of experiencing a radiation-related or genetic disease, for themselves or their family members, due to their nuclear test veteran heritage. This concept is explored in more depth in Section 4. Fig 21 shows that both nuclear test veteran and descendant respondents have experienced distress or concern, due to worries about radiation exposure. However, worries surrounding effects of any perceived radiation exposure are predominantly an issue for test veterans and spouses (38%), rather than for descendants (8%). This may be due to the lived experiences of veterans who have worked at nuclear weapon test sites increasing their perceptions of immediate risk. This phenomenon is explored in Section 4.
 Fig 21. The proportion of a) Nuclear test veterans and spouses, and b) descendants who have experienced distress or concern due to worries about historic perceived radiation exposure (%).
Fig 21. The proportion of a) Nuclear test veterans and spouses, and b) descendants who have experienced distress or concern due to worries about historic perceived radiation exposure (%).
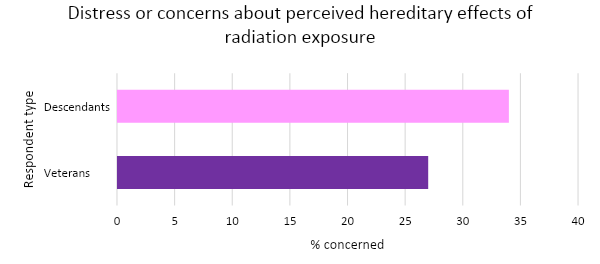 Fig 22. The proportion of a) Nuclear test veterans and spouses, and b) descendants who have experienced distress or concern due to worries about perceived hereditary effects of radiation exposure (%).
Fig 22. The proportion of a) Nuclear test veterans and spouses, and b) descendants who have experienced distress or concern due to worries about perceived hereditary effects of radiation exposure (%).
Both nuclear test veterans and descendants have experienced challenges in accessing high-quality information and resources about nuclear weapon testing, and any long-term health effects. While respondents identified with a variety of resources for support, as shown in Fig 24, undoubtedly this does not represent the full spectrum of support that could be available, and this lack of knowledge may leave this community without the support that they need.
 Fig 23. Reference materials currently used by nuclear test veterans and descendants to understand their nuclear test veteran heritage (%).
Fig 23. Reference materials currently used by nuclear test veterans and descendants to understand their nuclear test veteran heritage (%).
Fig 23 shows the differences in reference materials used by nuclear test veterans and descendants to explore their heritage. The purpose of this question was to understand what public domain information is used by this community, and to identify if the calibre of this information is of sufficient quality. The most commonly used resources reported by nuclear test veterans included a combination of books (75%), tabloid news (61%), and social media (56%). The most commonly used resources reported by descendants included books (75%), Wikipedia (71%), academic literature (43%) and social media (43%). The least popular resource for both groups of respondents was broadsheet newspapers.
More veterans than descendants are unsure about what resources to use, when exploring their heritage, and some nuclear test veterans reported choosing not to explore their heritage at all. One questionnaire respondent specified using National Archive resources in ‘other comments’. However, this has not been included in the questionnaire analysis as the National Archives are a publicly accessible, but expensive and not widely-available resource.
 Fig 24. Respondent identification of support resources (n = 198).
Fig 24. Respondent identification of support resources (n = 198).
Fig 24 shows that the most commonly identified resources for support provision among respondents are the BNTVA, Fallout (Facebook group), GP and other NHS services, the MOD, and Fission-line. The responses to this section of the questionnaire suggest that greater formal provision of centralised support is needed for both nuclear test veterans and their descendants. NCCF activities are beginning to fill a broad portion of this centralised support need.
-
Conclusions
The wellbeing and lifestyle questionnaire has provided useful quantitative insights into nuclear test veteran and descendant comparative life experiences, by exploring relationships, physical health, mental health, welfare and wellbeing, lifestyle, caring and care and hereditary concerns across the respondent cohort. It provides a guideline for further research, and raises issues that are explored in more detail through ethnographic and interview approaches. The results of this further qualitative study are presented in the next sections of the report.
-
Interviews
Themes that emerged from the interview data included veteran health and safety culture, disability, contested diagnoses and un-medicalised conditions, and mental health challenges. This section includes anonymised quotes from individual members of the nuclear community that are representative of themes that have emerged across the interview series. Any identifying characteristics have been removed, to protect participants identities.
Among descendants, the Nuclear Families study has identified self-reporting of mental health challenges, autoimmune conditions and somatic conditions, compared to the average population. This included a high prevalence of depression and anxiety, autism and learning disabilities; autoimmune conditions included non-ionising radiation related thyroid autoimmune diseases, rheumatoid arthritis, multiple sclerosis (MS), and inflammatory bowel disease; and conditions such as fibromyalgia and Myalgic Encephalomyelitis (ME). These conditions are not associated with ionising radiation exposure, but have the capacity to be disabling and therefore have a significant impact upon the wellbeing of the children and grandchildren of veterans.
There were also instances of congenital defects, including effects to hearing, bone structure, and syndromes reported. As this study is self-selecting, this indicates an avenue where further research should be undertaken to gain a deeper perspective of the meaning of these reported figures. This study provides qualitative insights into the considerable impacts to quality of life that have been experienced by members of the British atomic veteran community. However, it is not a prescriptive guide or necessarily reflective of national statistics overall.
-
Veteran health and safety culture
It was important to gain insights into the historic health and safety culture that surrounded the experiences of the nuclear test veterans, as this informed their overall perspectives of the experience. It is also notable that a culture of secrecy surrounded the nuclear weapon tests, meaning that individual veterans would undertake work without being provided an overarching insight into its wider significance or impact, from either health-related, geopolitical or cultural perspectives.
Veterans, as well as their wives and children, explored this topic to discern if there were differences in information shared to families, compared information shared with interviewers by the nuclear test veterans, and to identify any reasons why this information might be different. While some veterans enjoyed their time on the island, others found the lax health and safety culture concerning. It is noteworthy that family members often knew less about their veteran family members time working on the British nuclear weapon tests than was disclosed to interviewers. This may be representative of the culture of secrecy that pervaded at the time, meaning that family members could not be told of their work. It may also represent an attempt by nuclear test veterans to protect their families from any bad experiences that they may have had during their participation in the nuclear weapon tests.
Sheila, a nuclear test veteran’s wife, described her concerns about the health and safety culture of her husband’s work at one of the messes [dining halls] during Christmas Island nuclear weapon testing.
“When he was working in one of the messes, one of the cooks used to throw the dirty pots and pans back at the washer uppers, and this particular day he had three lunches on his arm. He was going to walk through a door, and a knife went passed his nose; thrown at the washer upper, by the chef.”
She expressed concerns that this lax health and safety culture could have prevailed across roles and affected her husband’s safety during his time on Christmas Island.
Nancy, a nuclear test veteran’s wife, described her limited understanding of her husband’s experiences of Christmas Island.
“Well, on the island as he was post office trade he did the post office so there was no actual… The only thing he ever tells me is about when the bomb went off or came down or whatever, you know, they were all made to sit with their back to the act and what happened but, no, he never really commented about it.”
George, a nuclear test veteran, described unsafe fishing practices, another aspect of a very liberal health and safety culture on Christmas Island.
“We used to catch the sharks for them, because we’d use a Land Rover, a long piece of steel wire rope, some bait on the end of the hook, throw the hook over the reef, and when the shark bit, drive up the beach and the shark would come flying out of the water…I didn’t witness but I know one fellow who went near the shark before it was dead and got bitten by a shark on dry land.”
Barry, a nuclear test veteran, described his stark first impressions of Christmas Island as an underdeveloped and contaminated place when he first arrived before any testing was undertaken.
“Disembarked at the plane: misery. It is not the South Seas Island where palms are waving, and white beaches and everything like that; it was just dirty, smelly, lots of flies.”
Barry proceeded to elaborate on the challenges of living there during the first phase of nuclear testing set-up.
“The accommodation was terrible, the tents were in tatters because of the… There was a high level of humidity there all the time, 90% plus, and very hot as well; so injuries or cuts or anything like that very quickly went septic. What else? The food was awful”.
The incidence of coral sores was discussed extensively by Christmas Island veterans, who said that injuries usually occurred during football. Maurice described the treatments that were provided for injuries of this nature.
“Now, the one thing on Christmas Island that you did, we had a very, very active football league there, but it was non-contact football, and if you got a cut of any sort, anywhere, you had to go to the hospital when the game was over, and it was scrubbed and disinfected.”
When the interviewer asked why this treatment happened, Maurice clarified that it was due to the toxicity of the coral, and that he perceived this toxicity to be related to ionising radiation exposure.
“Now, whether the coral is poisonous anyway, but they knew, back in HQ in the UK, that it was infected coral. Contaminated coral… The nuclear waste. Fallout.”
This contrasts the experiences of later tours by servicemen to Christmas Island. For example, nuclear test veteran Harold described his experiences more positively, but expressed concerns about the toxicity of his environment.
“Well, I have to be honest, when we got there the living accommodation was excellent, the food was excellent. I was in the company of guys who I liked. We had a whale of a time. But what we didn’t know, the buggers were poisoning us at the same time.”
Akin to other veterans, Christmas Island veteran Frank described DDT being sprayed on the camp to protect the servicemen from mosquitos. He expressed some concerns about the long-term effects of this treatment.
“No symptoms, even being sprayed twice a day with DDT, that didn’t affect me at the time. I don’t know if it did affect me, but we were sprayed, morning and night, with DDT from the air, by an aeroplane, a small aeroplane. But I just got on with the job.”
Christmas Island veteran Roger described his experiences of spending recreational time about half a mile away from ground zero, and the lack of any health and safety signage in the zone.
“And there were no notices, there was nobody there to say you can’t go. There was nobody there to say get out and go back to your camp. We were just allowed to go there. We used to go down to it across the lagoon.”
Roger also described illicitly eating fish and chips made from the left-over bycatch that was provided for scientists on the island, and that should have been given to islanders.
“What fish the scientists didn’t want to take with them we gave to the natives to eat, and we were not told to eat the ones that we kept, which one of our cooks at the time, Ken Taylor, who did work in the galley, he had a fish and chip shop going. So, all the port camp and some of the top camp used to come down for fish and chips.”
This represents a difference in health and safety standards for servicemen and indigenous people on Christmas Island. Other nuclear test veterans reported similar scenarios of ignoring the scant health and safety standards that were in place. Herbert described looking into a container that was labelled “Do Not Touch”.
“One day, us landing craft crews went down to the big pontoon with landing craft along the side, and on it was a big container about that round and all these marines were looking at it. And it said on it, “Do not touch”. Well, what’s the first thing you’re going to do? So they took the top off; I looked over their shoulder and it was radioactive waste inside.”
Fred, a Christmas Island veteran, described the amount of time that he thought servicemen were stationed, considering whether those stationed for longer had a more difficult time.
“…because I know some who’ve gone 12 months, some who’ve gone 18 months, and then the ones who had the shortest stints tend to be remediation.”
Fred also mentioned the nature whereby radiation risk was communicated to servicemen, sharing assurances that no exposure could occur.
“What radiation? There wasn’t any, they told us. Gone.”
The health and safety culture was described simply by Henry, a Maralinga veteran, who when asked about health and safety briefings, replied.
“No. There was no Health and Safety aspect at all”.
These conditions would not have been reassuring, as they represented a wider lax health and safety culture at the time of the nuclear weapon tests. John, a veteran, described how members of staff died during his time on Christmas Island, but was not able to provide specific information as it was not discussed any further during his time there.
“We lost three chiefs out there in the first year, but there’s nothing ever been said about that.”
Ralph, a Maralinga nuclear test veteran described his attire during the nuclear weapon tests in Australia, and expressed concerns that any protection from potential exposures were limited.
“…on the day of the bomb we dressed in ordinary long trousers, long sleeved shirts; and that was our protective clothing, which was just normal stuff; it’s not protective clothing.”
However, Edmund, a Christmas Island nuclear test veteran, described the measures in place before the Grapple Y hydrogen bomb was detonated offshore of Christmas Island. He talked about a drill that was practiced by everyone on the island three times before the bomb was detonated. Other veterans referenced this scenario, but were also unable to provide more specific details of these events.
“Essentially, everybody was gathered to a point where they were able to be accounted for, we went through the whole drill, they used some conventional weapons to simulate the sound of the bomb; and so we were all gathered. We had the drill of what to do over the PA system: sit down, away, back to where you are, sit down. We had dark glasses, we had sweat rags on over the dark glasses, we had our hands over our eyes like that, and you were sitting, and then you drew your knees up, and you put your head on the knees.”
He proceeded to describe an evacuation strategy that was in place to move everyone to the south of the island if things did not go according to plan.
“…and there was sufficient transport available to take everybody to the furthest point on the island, had things gone wrong. So there were trucks there, we were all allocated a truck, we knew which truck we had to go to…“
Edmund also described the aftermath of the Grapple Y test, and its effects to local infrastructure.
“…It blew down the air traffic control tower, it blew a lot of tents down, it blew a lot of the laboratories down, where the AWE were. Were the blasts were such that anything that – you know, it was so intense, itself, that if there was a solid object, it just blew down, I suppose.”
He described the effects to local wildlife and marine life.
“The dreadful thing was, the birds were blinded, those seabirds…the birds has been blinded… A lot of birds dead, but about ten days afterwards, we went down to the actual land point nearest to the explosion, and there was just a mass of sea life, rotting sea life, all over this point; and all the earth was scorched as well, quite badly.”
Edmund said that the reasons why the creatures were there were not discussed. This provides important insights into the cultures of health and safety and secrecy that prevailed during the time of the British nuclear weapon tests and the early Cold War more generally. This could have contributed to current veteran and family members perceptions of risk.
Bertie, a nuclear test veteran, described the hierarchical nature of his time on Christmas Island.
“I got on as you would expect or as I expected; I did my job, if there’s anything to do with my job and I had to make the decision, I expected people to obey the orders, whoever they were.”
This echoes the sentiments of other veterans across ranks and forces, and suggests that there was not much space to contest or discuss the purpose of orders and their health and safety outcomes.
Martin, a Christmas Island veteran, described his experience of viewing the Grapple Y nuclear weapon tests. His experience reflects the confusion of veterans of both Grapple and Maralinga tests, in not understanding the implications of what they had just witnessed.
“Well, it was absolutely dreadful, because you couldn’t comprehend at that time exactly what had happened.”
Dennis, a nuclear test veteran, described hierarchical differences between the treatment of himself as a low-ranking member of the military and his commanding officer (OC), after a visit to Christmas Island’s Ground Zero zone. He described a decontamination and monitoring process that he was provided, but said that similar concessions were not made for his OC.
“I said, “Look, you’ve done all this to me here, my land rover is washed all done, yet my OC got out of my land rover still will all the dust and muck and everything he’d got on him and walked straight in to his officers’ mess”. “Don’t you worry about your OC” he said, “Just worry about yourself corporal, we’ll deal with your OC”. Now why did they let him go back in there without cleaning himself down when they did all this decontamination with me? Now unfortunately, my OC is dead; he died of cancer. I didn’t; I didn’t get cancer.”
Dennis also described what he perceived as long-term health effects to his OC, as a result of this different treatment.
In common with several other nuclear test veterans, Edgar was concerned about state monitoring after his participation during the Christmas Island tests.
“And, I said then that really I think now, the reason why that was – MI6 carried out a test on me when they’re dealing with me –“
It is plausible that post-test state monitoring could have occurred, but it is unlikely that this work would have been undertaken by MI6. Veterans described how they were unable to talk about any traumatic or challenging experiences that occurred during their nuclear service. This is exemplified by nuclear test veteran Oliver’s decision not to talk upon returning home from the tests.
“No, because for one thing, we were under the Official Secret’s Act, we weren’t allowed to talk about it. And you have got to remember, I was in the military at the time when I came home, so definitely I wouldn’t talk about it.”
Thus, the lack of information provided to this community have meant that they have had to create their own understandings of their experiences. To conclude, this section provides an insight into the precarious lives of the nuclear test veterans during nuclear weapon testing, and their experiences of a challenging health and safety culture during the nuclear weapon tests, as they were exposed to a variety of hazards beyond ionising radiation from the nuclear weapon tests.
-
Disability
The atomic veteran community faces challenges in accessing general healthcare, mental healthcare and social support services, and in obtaining formal recognition of their status as British atomic veterans and atomic veteran descendants by healthcare or state. They suggested that this could be due to a lack of knowledge of the challenges of the community by health professionals. Both disabled veterans and disabled descendants reported feeling unsupported by State disability provision, with particular challenges arising pertaining to gaining the disability allowances that they are entitled to. Members of the community stated that challenges arise in this domain due to the complexity of documentation, and lack of recognition or support for documentation of their health challenges by healthcare providers or state. It is normal for high disability prevalence to occur in aged cohorts, as age-related conditions arise. Among the nuclear families study group, disability was as expected among aged veterans. However, the self-reported instance of disabling conditions was slightly elevated among descendant respondents, and included rare and unusual hereditary conditions, in addition to common autoimmune conditions.
Disabilities relating to the joints, skin, bowel and lungs were commonly described by nuclear test veterans. Martin, a Christmas Island veteran, described his disabilities to an interviewer.
“I had a pacemaker fitted fifteen years ago, which is heart problems; I then had bowel cancer, but these could’ve happened anyway. And at the moment I’ve got fibrosis of the lungs. That could be a responsibility of Christmas Island but not necessarily. And that’s my health at the moment.”
Martin described the support that he received for his disability, and his condition’s life-limiting nature, as his partner concurred.
“I recently got a disabled badge through this breathing now it’s really got me bad. And that has restricted me. I’ve suddenly got so bad that I can’t do any work. I struggle, don’t I?”
Conversely, Dennis, another Christmas Island veteran, directly attributed his broken back, which occurred during a fall in 1985, to his nuclear test veteran service, and had gained medical confirmation that this was the case.
“Well, they just told me that I’d got radiation infection in my spine. I’ve got a high rate of radiation in the bone.”
When this was discussed further with the interviewer, Dennis clarified the situation and his firm belief that ionising radiation exposure was the reason for his broken vertebrae.
“Well, that I got radiation poisoning from Christmas Island. If I’ve got too much radiation in my body, where did I get it from? From Christmas Island because I was only on Christmas Island; I’d never been anywhere else with radiation.”
For some nuclear test veteran descendants, health challenges have been an ongoing concern. In one interview, Sally, a nuclear test veteran daughter, described her debilitating and unusual health challenges to the interviewer, and their impact on her working life.
“So, Dercum’s disease. I was diagnosed with that, and then my back went, and one particular day I had gone to work and they sent me home and said, ‘Don’t come back until it’s fixed, you can’t carry on like this”.
She explained that her health conditions had escalated over time to include multiple disabilities.
“So, I started the every other day injections of B12, and then the three monthly injections. I ended up seeing a podiatrist because my feet were so sore. Then, I saw a physiotherapist. Then, I got a prolapsed bladder in the meantime. So, this was sort of, everything was happening to me, I was just going downhill, downhill, something else, something else, something else.”
Sally was pessimistic about her long-term health prospects, and linked her condition to her father’s participation in the nuclear weapon tests.
“I think the only thing that could happen that could be worse than what is happening at the moment, is for me to have terminal cancer, but I guess, because we haven’t reached that stage in our lives yet as descendants, we have no idea what is going to happen…”
Sally went on to express altruistic concerns for the community, beyond herself.
“…None of us knew what was going to happen to ourselves now, you know. So, I guess we don’t know what is going to happen in the future. I guess, I am not the type of person who would sit and worry about it, but there are others out there that I know that do, it is a concern for them.”
Emily, a nuclear test veteran daughter, listed a variety of health challenges that she experiences which leave her incapacitated and unable to work.
“What have I got? I have a non-malignant brain tumour. My gallbladder had gone because I had gallstones. My saliva crystallises so I have stones come out of my cheek bones and my mouth, so that does hurt. And I’ve now got kidney stones. I have thyroid nodules. My thyroid runs just dead on top of high. Not enough to medicate this time, I won’t know for another six months, but have nodules on them. My throat. I had six tumours removed from my voice box and my vocal chords last year. But again, non-malignant. I have chronic asthma, or they call it severe asthma. Ignore the smoking. One doctor diagnosed I have double knuckles on my fingers, I have knuckles both sides, but then the next doctor just calls them extra-large knuckles. I have lumps on every finger on the inside and on the out. Which doesn’t really affect me but they reckon I probably will have horrendous arthritis when I get older. I have the same on my little toe, I have an extra lump, big lump there, it’s nearly like a little toe but it’s not quite a toe, it’s just a nodule, they call it… My teeth. My teeth started to rot in my early teens and I had them all capped, and it’s been ten, 15 years I’ve had false teeth at the front.”
Anita, a nuclear test veteran daughter, talked about the congenital health challenges that her family faces, considering some of the other factors that could have come into play.
“…my brother’s, one of my brother’s daughters, was born with a malformed hand and deafness, and then another one of his children died within a few weeks, I don’t know what of, I think she was premature. It is one of those things, like her mother would have smoked throughout the whole pregnancy, but yes so it does seem that there is quite a lot, out of all the children that have been born, there has been a fair amount of problems, considering, so yes, it has sparked that ‘oh I wonder if that is linked, that is weird’.”
There were health concerns described by veterans for their children. Alfie, a nuclear test veteran, talked about the challenges that his grandchildren had faced, with one having a hole in the heart, another having dyslexia and Asperger’s syndrome. He described how he thought these health problems were unconnected to his time working on the nuclear weapon tests.
“I don’t think it’s got anything to do with my service.”
-
Contested diagnoses and un-medicalised conditions
Contested diagnosis occurs when the individual experiences symptoms that are contested by medical professionals; whereas un-medicalised conditions are those that are not formally accepted or understood by medical professionals. Instances of both contested diagnoses and un-medicalised conditions occurred among descendant interview participants.
This section explores the challenges that are faced by nuclear test veteran descendants who live with un-medicalised conditions, contested conditions, and chronic health conditions including myalgic encephalomyelitis (ME) and fibromyalgia syndrome (FMS), unexplained chronic pain, and irritable bowel syndrome (IBS). These conditions are more common in women, and often express comorbidities of anxiety and depression (Monden et al., 2018). Patients with these chronic conditions face unique challenges accessing care outside of their homes, due to a diverse range of symptoms and physical limitations (Van Beugen et al., 2014).
In common with others, Helena, a nuclear test veteran’s daughter, described her challenges with exhaustion and talked about her difficulties in receiving a specific diagnosis for her symptoms.
“It’s been something I’ve thought about maybe going to the doctor for because it’s not like a tiredness, it’s a constant fatigue – even before I had children – it’s worse now I’ve got children. I get lots of pins and needles, sometimes numb fingertips, and drop things.”
Helena attributed her health challenges to her father’s service, as she described her good health and upbringing as protective factors against poor health.
“I can understand if I’d had a different background or I wasn’t looked after as a child. If I hadn’t had a good balanced nutritious diet I could possibly understand that.”
Alan, the father of a deceased descendant daughter, described challenges in medical professionals associating his daughter’s condition with his own experiences of being a nuclear test veteran.
“…doctors seem very reluctant to discuss anything when you approach the subject from a nuclear view”.
This veteran descendant described the experiences of their father, and the way that medical professionals created occupational and environmental linkages between his tuberculosis (TB) and his time as a nuclear test veteran.
“The chest consultant said that the TB was there, and was caused by a – he reckoned it was caused by a chemical they were using in the tests but it laid dormant for years, and it was only activated when he had this really bad chest problem with pleurisy, and it brought it to life”.
This describes the transformation from latent to active TB a bacterial lung disease that is not typically associated with chemical exposures, but could possibly have been transmitted to the veteran during service.
To conclude this section of the report, there are a diverse variety of disabilities among the nuclear test veteran family and descendant community. Some members attribute their family’s poor health to potential exposure from the nuclear weapon tests, whereas others consider luck, lifestyle or other hereditary factors to be more significant.
-
Mental health
Mental health challenges across the interview series, with descriptions of anxiety, depression and PTSD featuring among both veteran and descendant communities.
Humphrey, a nuclear test veteran, described how he has experienced a mental health “breakdown” after his service on Christmas Island, that was accompanied by excessive alcohol consumption.
“I can’t explain it. You know, I couldn’t work it out. It just went. I started drinking heavily and, you know, that was it, and it just fell apart. But as the years went by and it all went… everything quietened down I suppose and I carried on with my service life and that until I finished.”
An interviewer spoke to Eric, a Christmas Island nuclear test veteran, about his wellbeing, and he described his experience of mental health in colloquial and stoic terms.
“I feel a bit – okay, I’m quite, quite … I feel a bit down and down in the dumps every now and again but, you know, I get by, don’t I?”
Sheila, a nuclear test veteran wife, described her husband’s breakdown in the 1960s and his challenges in gaining employment with compassionate humour.
“It was just living with those dark moments when they appeared. The dark moments will always appear in life, but whether or not that was because of Christmas Island, but for Ron, it was the disgrace of being unemployed, and not able to support his family was the hardest thing he ever lived with, and this is when I turned round and said, “Well, this is why you had to marry a smarty pants, dear,” I said, “because she could keep you in the style to which we’ve become accustomed”.
Irene, another nuclear test veteran wife, described how her husband had become calmer over time.
“He’s a bit calmer now than what he used to be. He used to be not a whirling dervish but if he gets the bit between his teeth he won’t let things go.”
Veteran mental health challenges reported by descendants were often described in terms of violent or emotional outbursts, unpredictable behaviours, or witnessing marital discord in the 1960s and 1970s. Anita, a nuclear test veteran daughter, described how her veteran father’s mental health adversely affected his behaviour towards his family.
“I saw a lot of violence when we were children, towards my brothers, the difficult ones.”
Anita described these negative interactions to the interviewer in more detail.
“He was always very – seemed to be quite angry a lot, he was just very shouty, there was a lot of shouting, he was always shouting with mum and they were arguing all the time, but with us, it was like he was just the killjoy. He would come in and the atmosphere would change, and it was always better when he wasn’t there, basically”.
She described how she had sought private mental health therapy to help her to overcome the challenges that she had faced, and to reconcile her experiences.
“I have had … yes I went and had counselling through self-referral, private counselling.”
Brenda, a nuclear test veteran’s daughter, also described her father’s challenges, and the impact that this had on his first marriage.
“…and he wouldn’t admit anything. He wouldn’t get help from nobody. But to walk out of a marriage with three children, remarry, have three more children…”
This echoes other veteran descendants’ experiences of their father’s mental health challenges, including guilt and anxiety.
“I know he’s not anxious to talk about it, like he was. I wouldn’t say, it’s mental health, I’d just say it’s guilt through not knowing what was going to happen, and what would happen later on with everybody else”
Helena, a nuclear test veteran daughter, described her experiences of anxiety and panic attacks as a young woman.
“…and when I was younger, when I was a teenager, I had anxiety then and panic attacks – like getting onto the school bus I would literally be shaking and sweating and that type of thing. For a long time I couldn’t go into a social situation because I felt people were looking at me, and the sweats would come and I’d blank out and not see anything.”
This section of the report concludes with a suggestion that considerable further mental health support provision is enacted for nuclear test veteran families.
-
Awareness and support
This section of the report provides insight into the atomic veteran families’ experiences of awareness of their condition, by organisations such as the National Health Service (NHS) and the BNTVA.
The Nuclear Families study included questions that related to respondent’s experiences of receiving medical support, with the aim of providing insight into the current state of healthcare provision to this community. Many atomic veteran community members are satisfied with the quality of medical care that they have received, but have encountered a lack of medical understanding about the conditions surrounding the British nuclear weapon tests and their potential for health implications. A small but significant minority of study participants have encountered direct challenges and contestations of their health experiences by healthcare providers, in the context of their own health, but also the health of family members.
A test veteran, Marcus, described a lack of awareness of test veteran-specific health challenges, during an encounter with a doctor.
Marcus: “Yeah, yeah, I said I was a direct test veteran…and nothing was said about it.
Interviewer: Do you think they knew what a test veteran was?
Marcus: No, no, no. It never used to come up then.”
Another test veteran, Owen, and his wife, Olivia, described their experiences of medical recognition, or the lack thereof, of their occupational nuclear work.
Owen: “…I went to the doctors down here, and the doc…he was, and then I went to tribunal, didn’t I?”
Olivia: Nuclear never come up with the doctors or anything. Not a lot. It’s what we said about it. You know, Owen would say, ‘Well, I’ve been to Christmas Island, watched the bomb go off’, all that sort of thing’…But nobody ever said ‘was it to do with that?’”
A veteran wife, Sheila, described her understanding of the healthcare from a more cynical perspective, as her lack of response and explanation the medical profession has been interpreted as a cover-up.
“The thing is, you see, everybody in the medical profession were backing off anything to do with the nuclear industry. You know, it was as if they’d been warned off saying anything like that….It’s as if they’re trying to wipe it off the face of the Earth”.
This demonstrates the lack of general or common medical knowledge about the work of the British nuclear test veterans and their work. An NHS factsheet has been designed and included in Appendix 1 to aid in addressing this challenge. This report suggests that further information is distributed across relevant NHS services.
Veterans and their families may link their experiences and health conditions to nuclear exposure. However, there is limited awareness of the occupational and socio-environmental linkages of their health challenges by health professionals. This is despite an abundance of medical literature on the physical health challenges that may or may not arise in this community (see Section 1.3 for existing literature).
There appear to be three main reasons why there is less knowledge of the health challenges relating to British atomic veterans, when compared to, for instance, veterans with Gulf War Syndrome. The first reason could be in part be due to the inherently secretive nature of the British nuclear weapon test series, which means that medical professionals may be unaware of their occurrence and effects. The second reasons is scalar, as lack of knowledge may also arise due to the timescale of the tests being beyond the current lifespans of most medical professionals today, meaning that they have no personal memories of the tests to draw upon. Finally, there appears to be a need for improved ease of access to health guidelines for those who do treat the British atomic veterans and their families. Conversations with atomic veteran families demonstrated that their GPs in particular are very well-intentioned and well-placed to provide more specialist support to this community, but are poorly equipped with general information about the conditions associated with ionising radiation exposure and conditions associated with the UK Compensation scheme for radiation-linked diseases, as well as the psychosocial effects of intergenerational trauma. These challenges could be resolved by the provision of a well-advertised visiting specialist GP locum, and comprehensive ionising radiation and health information pack to all members of the nuclear test veteran community.
Humphrey, a Christmas Island nuclear veteran, and his family, described the challenges that they have faced in getting scientific support to help to contest the state’s decision, regarding their nuclear test veteran health status.
“All I want is my chromosomes looked at to see if it is me, because the read outs they get from chromosomes that have been coming from New Zealand which are not recognised in this country for goodness knows why, you know, it makes you very, very annoyed in the least to think that somebody in our commonwealth has suffered the same thing and they’ve got more information from their side, and when it comes over here it is all lies.”
He felt as though he could not trust the state to provide a true account of any exposure risks. Alan, a father of an unwell descendant daughter described the experience of supporting their daughter with diagnosis of and treatment for Cushing’s Syndrome, and the lack of NHS provision for the family.
“I spent seventeen weeks in hospital, I slept on the floor beside her bed, because they had no parental accommodation at the time”.
He described how this experience was repeated the following year, as treatment progressed. Alan explored the experience of trying to understand his deceased daughter’s medical reports, relating to death due to Cushing’s disease, which is often caused by a carcinoma of the pituitary gland, and then discovering that her medical records had been lost.
“Her death certificate just said a carcinoma. So that was void of information…they told me all the records had been lost, but for every day while we were there, before and after her operation, she was photographed”
A veteran daughter, Lizzie, described her challenges in discerning good information online.
“The resources can, I know, sometimes they frighten you…if the doctor tells you not to look something up, that’s the worst thing they can do….But, they say ‘don’t look it up’, so, you think, ‘I want to look it up’. Nature makes you do it”
However, there are also some positive descriptions of support and awareness. Alan, the father of a descendant daughter with Cushing’s, described his experiences of joining the BNTVA.
“…It wasn’t until I got involved in the association, then I realised that other people had got problems, not the same but very similar, and I thought there could be a connection with my attendance on the island and this situation”
This suggests that the BNTVA plays an important role in providing community support for those who have experienced intergenerational health challenges.
There is limited community awareness of the effects of nuclear test veteran heredity, of the effects of ionising radiation, and of the variety of options that are currently available for support, including funding from the NCCF. This report advises that more detailed and impartial guidelines are distributed to the nuclear test veteran family community about the nature of the nuclear weapon tests, the effects of ionising radiation, and options for seeking further financial, social, mental and physical health and care support.
-
Perceptions of Risk
There is an elevated perception of risk among the nuclear test veteran family community. This has manifested as a perception among participant families that there are links between intergenerational family illness, and that descendant’s health and wellbeing has been directly influenced by nuclear test veterans’ fathers participation in nuclear weapon testing. There is also a perception of hereditary effects to the community, and the belief that a long-term genetic legacy awaits immediate descendants and their further descendants. Accompanying these sentiments are uncertainty about the origins of health challenges among descendants, and concerns about future health challenges that may emerge.
One nuclear test veteran, Wilf, described his perspective on any future health risks to his children and grandchildren.
“Well, that does bother me a lot, especially with the grandchildren. Myself, no. But the grandchildren and my own children, yes. Have I left them with a time bomb?”
Another nuclear test veteran, Arthur, described his worries as being certain, and suggested that future medical research could help to allay his concerns.
“Only that there’s so little been done about the source of the problem, medically, and I know now there’s nothing more can be done for me, or my brother or sister. Whereas I’m hoping that sufficient research can be done to make their life easier.”
Nuclear test veteran wives and partners also expressed their concerns. In this instance, Gina linked those concerns to existing health challenges experienced by her grandchildren.
“Yeah, definitely. Definitely. Yeah, I do worry. I’m concerned that my three daughters have always looked after themselves, ate well during pregnancy, didn’t smoke, didn’t drink and, yet, three of the children have issues.”
A nuclear test veteran’s wife, Sheila, expressed concerns about her nuclear test veteran husband’s blood donations.
“…And, at one point, there was instructions that they shouldn’t be blood donors any more. But, if you ask them now, they’ll say, “No, no, no, no, no, no. You’ve dreamt that up”.
She was also concerned about any potential effects to others from his blood donation.
“I mentioned to you about him being a blood donor, and because he was a B rhesus negative, what damnations has he made to other people, as well?”
While this is not a plausible risk, it provides insights into the need for greater support and education among this community. Sheila also talked about how the medical profession and the state do not currently understand her concerns.
“Well, I worry about it, but there’s nothing I can do about it. So, we’ve just got to wait and see what happens, and hope that somebody believes you when you tell them there is a possibility.”
Concerns are intergenerational. One nuclear test veteran son, Luke, described his concerns about potential health effects.
“Yeah, I’m definitely concerned more for the ten-year-old out there, more than anything else, as to whether anything will affect him later on down the line.”
He went on to elaborate his concerns, with specific worries about sudden health effects to his son.
“You would worry that you’re passing on something generation to generation that could have a massive impact on, say, Sam’s [veteran grandson’s] life if I… if we pass something to him that meant that he ended up with a very severely disabled child in his life. That would have a massive impact on his life…That’s what I would worry, that there could be something that comes along suddenly.”
Irene, a nuclear test veteran daughter, talked about her concerns relating to hereditary effects.
“I think about it. Like dad worries about children and grandchildren, I worry about my children and my grandchildren and how far-reaching this could be.”
Ellen, a nuclear test veteran daughter, is concerned about future hereditary risks to her son.
“Yeah, I do worry. Obviously, again, it boils down to worrying about [her son] and what his children are going to be like –“
Jenny, a nuclear test veteran daughter, also described her own concerns, expressing issues surrounding uncertainty of any potential future health challenges and their origin.
“Well, I suppose you’re just annoyed really because you didn’t know about it, you didn’t know that you were perhaps genetically giving something to your own child or you’re passing it down through that child here and grandchild, it’s not fair really to not know. I mean if I’d have had a child that was, you know, severely disabled or something was that through the genetics of stuff, you know?”
She concluded with the following statement.
“It’s unfair that our father wasn’t told what he was being exposed to and what the consequences of it was, of what you could give to your own children, you know…I’m quite lucky that mine are quite healthy really but you don’t know do you?”
Alan, a nuclear test veteran who did not have children, described his lack of concern about any effects.
“Never concerned us because we haven’t got children”.
Helena, a nuclear test veteran daughter, expressed concerns for her brother, and questioned why her family had experienced health challenges.
“I’ve always questioned it particularly with my brother of, “Why is he like this?” And I think that’s left me with… I don’t know what any problems I’ve had have been inherited or whether it’s been a knock-on effect from him, if that makes sense.”
When Ellen, a nuclear test veteran wife, talked about her concerns, she discussed them in the context of her attitude to life.
“But, I’m not the kind of person that worries; I never really worry, you know? I’ve just got to get on with the housework.”
This sentiment was echoed by Nancy, another nuclear test veteran wife. Her perspective was that concerns should only arise if and when any hereditary effects are identified.
“I think there’s a multitude of different attitudes to take and I don’t think that necessarily one ought to be very worried, it’s about kind of gaging what’s…because we don’t have a full understanding of the situation anyway so my attitude is always, well, what’s the point in worrying if you don’t know yet. If we find from a genetic study that there is significant hereditary defects then we can all start panicking but until then it’s hard.”
Oliver, a Christmas Island nuclear test veteran, described his approach of researching US archives and media to try and find out more information about any risk to himself and his family.
“Well, having received documents and papers from various parts of it that I’ve researched, the Americans claim that you take 1,200 X-rays immediately on one detonation. And that’s documented in some of the evidence and DVDs I’ve got from the library.”
This selection of quotes represent an overarching theme of intergenerational nuclear anxieties, relating the activities undertaken by nuclear test veteran fathers, but also a stoic attitude to any perception of risk among other members of the nuclear test veteran community.
-
Perspectives on Family Planning and Reproduction
Interviews and workshop outcomes with women in the atomic veteran community revealed that there is concern about intergenerational wellbeing. There are two significant ways that this affects the community:
- Veteran and veteran wives’ experiences of regret, guilt and remorse about their decision to have children. This is compounded by anxiety and concern about latent or future health challenges arising for their descendants.
- Veteran daughters and grandchildren demonstrating attitudes and making reproductive decisions that are usually associated with those with known hereditary reproductive risks (i.e. those with a family history of hereditary disease). This includes increased anxiety arising over having children, an increased need for neonatal and postnatal child monitoring and screening, and in some cases, deciding not to have children because of perceived hereditary risks.
However, these are not universal perspectives, and not all nuclear test veterans and their descendants are concerned about genetic or hereditary effects. It is notable that this risk is gender-biased among the children of British atomic veterans, with more descendant female respondents mentioning concerns about reproductive risks and hereditary defects than male respondents.
During one interview session, a nuclear veteran daughter, Holly, jokingly discussed her intent to inform medical professionals of her father’s veteran status, should she have children in future.
“Don’t get me wrong, if and when I do get pregnant, I’ll be like ‘right, I’ve got this, this and this, my dad did this, this and this, so please watch’.
Holly’s description links her health with her fathers and identifies her own experience and knowledge as a patient. In common with some other study participants, Helena, a nuclear test veteran’s daughter, described some of the reproductive challenges that she had faced with reproductive health.
“My blood just doesn’t seem to clot that quickly. I miscarried pregnancies and afterwards Polycystic Ovary Syndrome; although they don’t call it Polycystic Ovary Syndrome in my case, I think it’s Idiopathic Hyper-aneurism because I have cists on my ovaries – and one grew so large that I had to have my fallopian tube and my ovary taken away, they said it was like a five pound baby really. But I always have regular periods and conceive children quickly so that’s why they call it, instead of Polycystic ovaries, Idiopathic – which I think means unknown cause or something like that.”
Holly expressed concerns about the unidentifiable root cause of her reproductive illness, but did not directly attribute this to her nuclear test veteran descendant heritage. Other veteran daughters described their reproductive challenges, including Alice, who encountered difficulties during pregnancy and childbirth, and that she attributes to her father nuclear test veteran service.
“My first child was when I was 21. I had horrific morning sickness, just off-the-scale awful, whether I ate or not. The first scan revealed that she had spina bifida and hydrocephalus, so I terminated her at about 20 weeks….it wouldn’t of been medically viable”.
Alice also described some traumatic experiences of childbirth
“…he was born by forceps in the end. I had the pelvic problem with him, carpal tunnel in my wrists and pre-eclampsia. [my daughter] was an OK pregnancy, but she was an emergency caesarean. I tore my uterus and bled loads after, haemorrhaging. And [my son] was low in the pregnancy…I was literally washed-out, couldn’t do anything. He was born five weeks early, fully in breach, a category 1 emergency caesarean, and a life or death situation. I haemorrhaged after him as well.”
Parental concerns of reproductive fitness were also made evident. Janet, a nuclear test veteran wife, described her husband’s concerns for her own future reproductive health and wellbeing.
“Especially when there is, like, when Julie’s pregnant. He worries, like he’s, you know, “Oh God,” and then the next one, “I’m pregnant again.” And oh, you know, as much as you want to be excited because you’re having this new baby in the family you’re also terrified because you don’t know what’s going to be wrong with it. And it sounds awful.”
Instances of stillbirth were discussed by veteran partners. A Maralinga nuclear test veteran, Luke, described the experience of his wife giving birth to a dead and deformed child.
“Got married in ‘57, had a child ’58, and when it was born it was a lump of meat. You couldn’t tell if it was boy, girl, human or whatever.”
Another nuclear test veteran, Mark, blamed himself for his descendants’ reproductive health challenges.
“Oh yes. Yes. I take full responsibility for their conditions.”
Anita, a nuclear test veteran daughter, described her own and her sisters challenges with reproductive health and her sister’s daughters health challenges.
“I have had a couple of miscarriages and a stillbirth…”
She went on to provide more detail about other members of her family who had experienced challenges with reproductive health.
“Yes, my sister had I think at least one miscarriage, and her daughter Isabelle who you will meet has a muscle … it was a developmental issue in the womb, well there is a muscle missing which means she won’t have – one boob won’t develop in the same way so that is like a developmental thing in the womb.”
To conclude this section, the cultural and social impacts of nuclear test veteran heritage are evident, when family planning and reproduction are considered. Nuclear test veteran families and descendants expresses concerns about the possibility of any potential hereditary origin of health challenges, and described the challenges that they had encountered with reproduction, as descendants.
-
Hidden Care
Care is an important hidden element of the experience of being part of an atomic veteran family. A recent study by Age UK showed there are now nearly 1.2 million people (1,183,900) aged 65+ who don’t receive the help they need with essential daily living activities. This represents a 17.9 per cent increase on last year and a 48 per cent increase since 2010. Nearly 1 in 8 older people now live with some level of unmet need. It can be anticipated that formal care and healthcare support may not meet the standards needed to support the more specific needs of an aged nuclear test veteran cohort, and their families.
It is notable that the aged British atomic veteran community shoulders both the receipt and the provision of intergenerational care. The Nuclear Families study discovered that members of the community often have intergenerational care responsibilities, such as caring for grandchildren and their partner; or caring for a child with disabilities and their nuclear test veteran parent.
The most common forms of care are those undertaken by the wives and children of the atomic veterans. There is a gendered element to this care, as it is often the wives and daughters who undertake the greatest amount of work. Many of these daughters also have familial and work responsibilities, which add to the complexity of undertaking this care. However, there were also examples of intergenerational care of children and grandchildren with health challenges by members of the atomic veteran community. While this work is undertaken willingly, it can compromise a time that is usually designated for retirement, relaxation and self-care.
One aged Maralinga veteran, Herbert, talked about his experience of aging and needing care, and the support he receives from a professional carer on a day-to-day basis.
“I’m severely disabled now. I can fall over ten, fifteen times a day and I don’t know why, I just go. That’s why I’ve got Lucy over there [his carer]. As you can see she’s well-built, I’ve got something to bounce off”.
This demonstrates that his carer plays an important role in supporting his day-to-day care needs. One nuclear test veteran daughter, Irene, described her reliance on care to support both her physical and emotional wellbeing.
“when [Name of carer] is not with me I can understand how easy it is to become a recluse. I don’t feel like getting out. I get up in the morning, I have my toast and that, and I don’t feel like going anywhere, and I could sit here all bloody day.”
Much of the time, care responsibilities are undertaken by family because there is limited provision for state support. A daughter, Julie, talked about her experience of caring for her father, while not recognising the un-medicalised elements of care that she provides.
“…sometimes I’d take dad to the hospital when mum was at work, but no like ‘care’, as in, having to make sure that they do this or something. Just, like, if he had an eye surgery then I would look after him when mum was at work, but generally mum would do that”.
Julie talked about the type of care needs that her veteran father requires.
“He can be left to his own devices, it’s more of a helping hand”
One veteran, Bill, described the process whereby his daughter became designated as responsible for his care by medical professionals.
“She was noted as being my carer, they just left it to her”.
One veteran wife, Lucy, described her experiences of caring for her husband’s surgical scars.
“We did get a little bit of help from the nurses, some of them would dress it couple of times in the beginning and things, but it was a learning curve, I got quite good at putting the steri-strips on and making sure that the dressings didn’t get wet, that sort of thing, you know, helping him in and out the bath. It was quite funny, he got one leg stuck and he was trying to get in and out of the bath, and it was sort of, we found it quite funny at times, and then his back opened up…”
An aged veteran, Tony, and his wife, Susan, discussed how they care and look after each other.
“Susan and I look after each other…we’re getting older, you know, and some things I’m better at than she is, and vice versa. So, you know, it’s a partnership, isn’t it?”
Tony talked about his experiences of caring for Susan, with considerable empathy for her health challenges. Tony is not alone in being a veteran cohort member who has provided care for their wife in old age.
“I look after Susan when it’s necessary, because she’s had two major spinal operations. She’s also had the removal of a gallbladder and a hysterectomy. She suffers now because of the spinal operation, she was warned that there could be nerve consequences, which she is now suffering.”
He continued to describe her legacy of health challenges, explaining how they had occurred throughout their life together.
“…and she’s had shingles, and a stroke in 1993, then just after we came back from Holland she was diagnosed with Type 2 diabetes”.
However, there are also scenarios where veterans refuse family care and support, as they don’t want to be perceived as a burden or responsibility to their family (Holroyd-Leduc et al., 2016). Jasmine, the daughter of a veteran, described her father’s proud attitude towards receiving extra support.
“He wouldn’t admit anything. He wouldn’t get help from nobody”
A nuclear test veteran daughter, Lizette, described the extensive visits and trips required to support her son’s disabilities.
“Yeah, hospital appointments, doctors’ appointments…It used to be speech therapy. Physio… Eye appointments for Ethan, because, obviously, he now has to wear glasses, as well, because the muscles in his eyes relaxed through the hypermobility. Daniel wears glasses, because he’s got one eye that will pull in, rather than look straight, so when he concentrates he goes a bit (laughing), he looks a bit googly eyed.”
To conclude, there are a diverse range of hidden care needs within the nuclear test veteran family community, that are not currently being addressed by state provision. The burden of care often falls to female family members, including the wives and daughters of nuclear test veterans.
It is recommended that care needs provision is assessed more generically across the community. It is a recommendation of this report that further support is provided specifically to the daughters and wives of veterans, in the form of formal care provision, to improve the caring capacities and well-being of the women of this community, and offer respite, if needed, from caring duties. It is anticipated that this information will be recognised by the NCCF and a specific targeting of their Care Wellbeing and Inclusion fund should be investigated to address this.
-
Memorialisation and Death
This study has shown that memorialisation is an important element of British nuclear test veteran culture. There are two different elements to this memorialisation processes:
- The memorialisation of their experiences as historic members of the nuclear military industrial establishment, through large-scale events.
- The memorialisation of their deceased colleagues and companions, through individual memorialisation and funeral services.
The processes surrounding memorialisation are often paramilitary in nature, including ceremonies. The 2016 Re-kindling of the Flame; 2016 Old BNTVA AGM, and 2017 Old BNTVA AGM were analysed through overt participant observation, to understand the impact and benefits of memorialisation to the nuclear test veteran family community.
This study process showed that events of this nature offered aged veterans an opportunity to undertake social networking and reunions with both friends and family members. Many veterans and their families look forward to nuclear community events, as they offer a sense of community and belonging to participants.
-
Seeking recognition
The desire for recognition and memorialisation through the provision of a British Government medal came to light during in-depth interviews with the British atomic veterans and their families, and during the media at the time of research. The discussion of various forms of compensation and recognition arose during interviews with both nuclear test veterans and descendants, including financial compensation, better healthcare provision, a formal apology and a medal. However, the overarching sentiment across the community is one of desire for recognition, rather than financial compensation.
“It doesn’t really matter about the money. It’s the recognition that we were the veterans who served at Christmas Island for the Atomic Bomb” (Forces Network, 2018).
The possibility and denial of a medal for specific recognition of services to nuclear warfare was mentioned in eleven of the interviews undertaken during Nuclear Families research, hence its inclusion in this report. At the time of writing, the British nuclear test veterans currently do not have formal recognition of their service in this way by the British Government.
During the study timescale, it is notable that a widespread campaign to seek a medal for British nuclear test veterans featured prominently across the British tabloid and broadsheet media, including articles and features in the Mirror and the Daily Telegraph. The nuclear community facilitated these articles, as an opportunity to publicly share their experiences of being part of a nuclear test veteran family and to contest state descriptions of their experiences, health and wellbeing. The campaign is seeking a both a formal apology and a medal from the British Government. A BBC article published in 2018 gives a public description of the contestations and emotions of the British nuclear test veterans, as provided by Mr Douglas Hern.
“We have lived with the trauma of the tests and the consequences through our families and it would be nice to be recognised and valued for what we did for our country.” (BBC, 2018)
His quote demonstrates that there is a perception of effects to family life among the nuclear community. The MOD response to the British nuclear test veterans’ desire for recognition is one of gratitude and consideration, but it currently does not recognise any evidence that links participation in nuclear weapon tests to poor health among British nuclear test veterans or descendants. This has been echoed by descendants, but there is also an element of memorialisation to their discourse. Julia, a nuclear test veteran daughter, justified her desire for a medal to commemorate her father’s work in terms of memorialisation.
“I just want something that recognises my dad’s work. Something for us to remember him by and to pass on to our own children.”
The possibility of a medal providing a route for memorialisation of a nuclear test veteran father was echoed by other interviewees. It is tied into ways of sharing heritage with family members who may not have met their nuclear test veteran family member. Luke, a nuclear test veteran son, talked about the loss of his father and his desire to share his heritage with his son.
“My father died before my son was born. It would be so meaningful to have something to share with him, to help him learn about his grandad.”
This shows that the issue of seeking a medal is interrelated with family heritage and the long-term maintenance of collective memories and understandings of the nuclear test veteran family member. It is not just an object for the veteran to commemorate their own experiences by, but something for family members to pass down through the generations.
-
A “Good Death”
This section explores the significance of memorialisation and bereavement to the British nuclear test veterans and their descendants, and the need for provision of a good death and memorialisation process. It identifies that bereavement and memorialisation of the dead form an important element of British nuclear test veteran community culture. All surviving airburst test veterans are now aged, and their ability to prepare for a good death becomes increasingly significant to them and their families as time passes. The significance of their nuclear test veteran status can form a component of the memorialisation process, and is definitely integral to the bereavement process for members of the descendant community.
A “good death” consists of preferences for a specific dying process, pain-free status, religiosity, emotional well-being, life completion, treatment preferences, dignity, family, quality of life, and good healthcare (Meier et al., 2016). The long-term health challenges of nuclear test veterans, and the more widespread intergenerational geography of contemporary family life mean that it can be challenging to ensure that all these criteria are met. Several veteran partners and descendants talked about the quality of palliative healthcare, with mixed perspectives. Some have experienced excellent NHS care and support, whereas others feel let down. Anna had a positive experience of palliative care when their husband died, describing NHS care provision.
“Palliative care was very good. He was well-supported and had plenty of pain relief. It was a difficult time, but I know that he received the best treatment possible…I’m grateful to the nurses who looked after him towards the end, they were kind to us, they let me sleep beside him in the final days”.
This contrasts with the experiences of Betty, who felt that palliative healthcare support was fractured and lacked continuity, and believed that a more rapid diagnosis would have prevented her husband’s death.
“It took too long. The care he received was OK, but everything was so slow. It was a year before he received a diagnosis of terminal cancer, and by that point it was too late. He underwent some horrible surgeries, some horrible treatments, to try and buy more time. He was so sick, it was heart-breaking”.
It is not just aged veterans in this community who have died. Several respondents have experienced other family members die. Alan, the father of a veteran descendant daughter, described his experiences of his daughter dying from Cushing’s disease.
“…It was in 1975, when she died. To me, the doctor at home knew a lot more about it than the doctors at hospitals were letting on, because he actually gave me a day and a time when she would die.”
It is evident that dignity and quality of life are both significant to the experience of death. It has been identified by this study that a “good death” is more challenging to achieve when the believed cause of illness is subject to contestation.
Bereavement was a topic that cohort members explored during workshops and interviews. Several cohort members described the pain and confusion of losing a father to illness while young, and later challenges associated with forming a family identity and of understanding their own heritage, as part of the bereavement process. Charlie described the experience of losing his father as a young man.
“We lost him too soon after a sudden and abrupt illness. I was so young, I have glimpses of memories of him. I wonder what it would have been like to have spent more time with him. I miss him. I also miss the man that I never knew…”
Ellen talked about what it was like to lose her father and how it affects her everyday life.
“I miss him every single day. I still talk to him even though he’s not here, I miss him…I can’t find the words to explain what it’s like to watch a loved one just slowly degenerate. It was painful for the whole family”.
Other descendants and veteran wives talked about the experience of losing a father later in life to chronic long-term illness, and described their guilt at feeling relief being released from caring responsibilities.
Dennis described the experience of providing end-of-life care for his elderly father, and how it restricted his day-to-day life, as he put his test veteran father’s needs first to ensure his final years were not spent alone.
“Yeah, it was tough. It was really hard when he died. But after years of caring for the old man, towards the end, it was almost a relief, you know?”
The BNTVA and NCCF play an important role together in the provision of bereavement care to the wives and descendants of nuclear test veterans, through events and community kinship and support. Online Facebook groups such as BNTVA and Fallout provide a place for some families to share their experiences of bereavement and grieving. These online groups have administrators who have personal experience of losing their veteran fathers, and use their own experiences in their capacity to help other members to place and process their grief. These online groups also offer a space for memorialisation and networked exploration of personal histories. This includes posts about the lives and experiences of deceased veteran fathers, and posts that hep group members to seek out other veterans who may have known a deceased father, to learn more about his life as a young man, for instance.
NCCF has been running and financing remembrance and memorial events for the entire nuclear community, not just BNTVA members, since 2017, and has provided over £220,000 of Care and Wellbeing support to both BNTVA and Non-BNTVA members of the British Nuclear Community during the time this report was researched and compiled.
Together, the BNTVA and NCCF also support open events and memorialisation ceremonies, as discussed in Section 3.5. These ceremonies offer a place and community for veteran wives and descendants. Ethnographic work undertaken during the Rekindling of the Flame in Paris, July 2016 and Kiritimati in April 2018 demonstrated that veteran wives and widows are included, welcomed and supported at these events. Of particular note was the support of an aged veteran widow who attended the 2016 Rekindling of the Flame. During this event, many of the veterans took time to chat to this lady and to make her feel included and part of the veteran community. She travelled to the event with family friends and described the experience as
“…very positive, everyone was very kind. It was such a special event”.
This captures the inclusive nature of British nuclear test veteran memorialisation, but also highlights its significance to maintaining social networks and support for aged veteran widows.
The BNTVA and NCCF also create a space for veteran wives and children to process their experiences at annual AGM events in the UK. These events are well-attended by the descendants of veterans, who run their own sessions to support their community and share their experiences. This provides an opportunity for an otherwise geographically disparate group of people to bond and share their experiences, increasing support and kinship, and helping to create a community that shares the experience of nuclear test veteran family bereavement.
For the families of the recently deceased the BNTVA offer a funeral service to support the families of the deceased[3]. This involved the provision of a standard bearer and BNTVA flag, a coffin drape, and delegate sent to provide words of support. The purpose of this post-life support is to demonstrate support for the families of veterans and show that the community still cares about them and their families. A veteran standard bearer representative described the experience of attending funerals as poignant, and important to the kinship of the community.
“Other people might forget them, but we don’t. It can be emotional – you see relatives who come and thank you, it means a lot to them, so you do it. We do it to support the bereaved relatives of the veterans”.
The aim of this voluntary and free services is to show respect to the person that has died and their family, and to demonstrate that they still have a community who will honour, respect and remember them. One of the challenges faced is ensuring that the families of the deceased are aware of the support that is available to them.
-
Conclusions: Looking to the Future
This section of the report provides an overview of research findings and offers potential avenues for future research with, and support for, the British nuclear veteran family community. This report has reviewed existing literature pertaining to this cohort and developed a mixed-methods approach to explore health and wellbeing, perceptions of risk, hidden care, and memorialisation and death.
It is anticipated that with the finalisation of the various strands of research funded through the NCCF, further Care, Wellbeing and Inclusion support gaps will be formally identified. These gaps will not only inform NCCF policy but can be used by all organisations operating within the Nuclear Community to engage, in particular, the Department for Health and Social Care illustrating their responsibility to address various challenges.
The British nuclear test veterans and their families have faced over sixty years of uncertainty pertaining to their health and wellbeing. This uncertainty has created an element of intergenerational anxiety across the community. This is due to a lack of centralised and high-quality information provision, relating to radiation effects, radiation protection, hereditary risks and similar topics.
The descendant cohort reported a slightly higher prevalence of autoimmune conditions, such as rheumatoid arthritis, autoimmune thyroid disease, asthma and skin conditions such as eczema. The community does include some members who reported rare diseases, but these do not occur in excess. The community also includes some members who reported birth defects, but again, these do not occur in excess. The most notable and concerning effects to health and wellbeing relate to somatic conditions and mental health. Many descendant cohort members reported experiencing debilitating conditions such as ME and fibromyalgia. Most noteworthy was the incidence of mental health challenges among both veterans and descendants, including anxiety, depression and PTSD. Many descendants linked their concerns about radiation-related illness and hereditary effects to their anxiety. This report suggests that further and more detailed statistical work is undertaken on a larger scale, to understand the relevance and implications of autoimmune conditions, somatic conditions and mental health conditions to this cohort. This report also suggests that a dedicated telephone counselling service is set up, to provide support to veteran descendants on matters such as reproductive and hereditary risks, mental health and wellbeing, and bereavement. Further to this, an NHS factsheet should be provided across Great Britain and Scotland to ensure that GPs have insight into the specific challenges that currently face the veteran and descendant communities.
Perceptions of risk have had an effect upon the descendant’s mental health, and in some cases have affected their life outcomes. Some descendants have undertaken perceived genetic altruism and decided to not have children due to their perception of risk. Other members of the veteran community reported not having had children due to health challenges or caring responsibilities limiting their opportunities to meet a partner and have a family of their own. Intergenerational hidden and informal care has had a significant effect upon this community. There are aged veterans who care for their wives, children and grandchildren. There are aged veteran wives who support their husbands and their husband’s children from previous marriage. There are veteran wives who care for their disabled adult children, and of course there are many descendants who take on a caring responsibility as their parents become older. There is an urgent need for better care provision and support for this community, to ease the challenges of informal care and provide respite for carers.
This report also explored the role of memorialisation to help the veteran community process and reconcile their experiences, and share their past with family members. It also explored the motivations and reasons why veterans are seeking a medal for their work, and identified this as a priority, in addition to recognition of their work. Memorialisation is an important experience for the veterans and their families, and this report identifies nuclear community events as a priority for community support. Finally, this report suggests that the nuclear community are provided with more support to facilitate a good death for less economically advantaged members of the nuclear test veteran community, and to help the community to memorialise their experiences more widely across the UK and beyond.
Appendices
Appendix 1: NHS information card template
Guidance Factsheet: Nuclear Test Veteran Families

This factsheet provides an overview and guidance on good practice for the support the specialised healthcare needs of the British nuclear test veterans and their families.
What is a British nuclear test veteran?
The British nuclear test veterans (also known as atomic, Maralinga, Grapple Dominic and/or Christmas Island veterans) are a unique group of servicemen who provided support to the British airburst and ground-level nuclear weapon test series during the 1950s and 1960s.
These tests followed the deployment of Fat Man and Little Boy atomic bomb nuclear weapons by the USA on Hiroshima and Nagasaki in 1945, as the UK sought possession of its own nuclear deterrent. The term ‘test participant’ has a particular definition in this context and includes servicemen present at the due dates, at any of the following test sites and experimental programmes.
|
Operation |
Site |
Date |
|
Hurricane Mosaic, Totem Buffalo, Antler Minor trials Grapple X Y Z, Brigadoon Grapple RAAF Pearce RAAF Edinburgh |
Monte Bello W Australia Emu Field S Australia Maralinga S Australia Christmas Island S Pacific Malden Island S Pacific W Australia S Australia |
1952-June 1956 1953-August 1957 1955-August 1967 June 1956-June 1964 1956-June 1964 May-August 1956 Aug1956-Nov 1960 |
There is no requirement for presence at detonations for nuclear test veteran status.
The British nuclear test veterans were young servicemen in their teens and early twenties at the time that work was undertaken and often did not have further education, academic or scientific backgrounds. A culture of secrecy surrounded their work. The average age of a nuclear test veteran in 2019 is 81 years old, and there are approximately 2000 aged nuclear test veterans still alive today.
The British nuclear test veterans undertook military support work to ensure that the development and detonation of the atomic bomb and hydrogen bomb tests were successful, Nuclear weapons are radioactive weapons of mass destruction (WMD), and many nuclear test veterans believe that their work may have left them at an increased risk of exposure to ionising radiation, beryllium and other toxic contaminants during their course of duty. It is currently considered by Public Health England that almost all the British servicemen involved in the UK nuclear tests received little or no additional radiation exposure as a result of their participation in the British nuclear weapon testing series.
Who are the descendants of the British nuclear test veterans?
Descendants of the British nuclear test veterans are described as their bloodline children, grandchildren and great-grandchildren. The reason for this specification is due to the perceived hereditary effects of ionising radiation. It is known that high-level exposure to ionising radiation can induce long-term genetic effects. Challenges with discerning the likelihood and quantity of any historic exposure, and therefore any potential dose to this community, have meant that it is not possible to infer any specific occupational health effects or the likelihood thereof, from the British nuclear test veteran’s participation in nuclear weapon testing. This scenario is a global issue, with the same challenges affecting aged veteran families of other nuclear weapon possessor states, including the USA, France, Russia, and China.
The nuclear test veterans and their families’ experiences of health have historically been surrounded by uncertainty and contestation, due to the perceived long-term physical and hereditary health risks of their historic work. Concern surrounding the long-term outcomes of their own and their children’s work may impact on their general wellbeing.
What challenges do this community face?
Historic studies have shown that any long-term physical health effects or risks as a result in participation in nuclear weapon testing are difficult to isolate or discern, due to confounding lifestyle factors and the advanced age of the nuclear test veteran cohort. Genetic studies are currently in place to try and identify and isolate heritable effects, if any. Psychosocial studies have shown that there are cultural, social and mental health effects to being a British nuclear test veteran or family member, due to the perceived burden of uncertainty surrounding long-term health effects.
Recent research has shown that there is a self-reported legacy of historic post-traumatic stress-like symptoms among nuclear test veterans; an increased frequency and incidence of family breakdown among the nuclear test veteran community more generally; and an increased incidence of self-reported anxiety and depression symptoms among the descendants of British nuclear test veterans. It is advised that members of British nuclear test veteran families who experience concerns relating to their heritage and health are referred to specialist genetic counselling services, if they are available. It is also advised that general mental health and social support services provision is made available for this community, by referral or other means.
Academic Literature
Alexis‐Martin, B. and Davies, T., 2017. Towards nuclear geography: Zones, bodies, and communities. Geography Compass, 11(9), p.e12325.
Trundle, C., 2011. Biopolitical endpoints: Diagnosing a deserving British nuclear test veteran. Social Science & Medicine, 73(6), pp.882-888
Muirhead, C.R., Kendall, G.M., Darby, S.C., Doll, R., Haylock, R.G.E., O’Hagan, J.A., Berridge, G.L.C., Phillipson, M.A. and Hunter, N., 2004. Epidemiological studies of UK test veterans: II. Mortality and cancer incidence. Journal of Radiological Protection, 24(3), p.219
Muirhead, C. R., D. Bingham, R. G. E. Haylock, J. A. O’hagan, A. A. Goodill, G. L. C. Berridge, M. A. English, N. Hunter, and G. M. Kendall. 2003. “Follow up of mortality and incidence of cancer 1952–98 in men from the UK who participated in the UK’s atmospheric nuclear weapon tests and experimental programmes.” Occupational and environmental medicine 60, no. 3: 165-172
Roff, S.R., 1999. Mortality and morbidity of members of the British Nuclear Tests Veterans Association and the New Zealand Nuclear Tests Veterans Association and their families. Medicine, conflict, and survival, 15, pp.i-ix.
Muirhead, C. R., A. A. Goodill, R. G. E. Haylock, J. Vokes, M. P. Little, D. A. Jackson, J. A. O’Hagan et al. 1999. “Occupational radiation exposure and mortality: second analysis of the National Registry for Radiation Workers.” Journal of Radiological Protection 19, no. 1: 3.
Links to Other Sources of Support:
Health Protection Agency website http://www.hpa.org.uk
NCCF website https://thenccf.org/
Atomic Weapons Establishment: http://www.awe.co.uk
Veterans UK website (including War Pensions): http://www.veterans-uk.info
Appendix 2: “’It was a Blast!’—Camp Life on Christmas Island, 1956–1958.”
Alexis-Martin, Becky. “’It was a Blast!’—Camp Life on Christmas Island, 1956–1958.” Environment & Society Portal, Arcadia (Autumn 2016), no. 19. Rachel Carson Center for Environment and Society. doi.org/10.5282/rcc/7693
http://www.environmentandsociety.org/arcadia/it-was-blast-camp-life-christmas-island-1956-1958
The 1958 US–UK Mutual Defense Agreement instigated nearly forty years of cooperative nuclear weapons testing, which only eventually ceased due to the implementation of the Comprehensive Nuclear Test Ban Treaty (CNTBT) in 1996. However, prior to 1958, the Grapple H-bomb nuclear test series demonstrated that the United Kingdom had sufficient technological collateral and a hitherto unrecognized influence upon the Cold War dynamic. Whilst the Grapple series were a bombastic display of British military prowess, there is a paradoxically human element to nuclear weapons testing. Here, we consider the day-to-day experiences of the soldiers who travelled to Christmas Island to test the bomb.
Due to the necessarily covert nature of the United Kingdom’s nuclear program, many of the soldiers were unaware of the political significance of their work. There was also little prior warning before deployment, one veteran said, “I was notified a week in advance. I was told to go to London airport with my entire kit bag … we were men with overcoats and gloves, travelling to a tropical island.” The soldiers were travelling prior to the advent of affordable commercial flight, and being posted to Christmas Island was often their first opportunity venture abroad. Most travelled by commercial aircraft to the United States and Hawaii, then on to Christmas Island. However, the Royal Engineers commissioned a commercial cruise liner to deploy their regiment, which also included the families of currently posted soldiers for a tropical holiday. Whether this was a compassionate gesture or a publicity stunt is subject to debate.
Upon arrival, the men initially bunked up in three-berth transit tents before relocating to larger facilities at base camp. Accommodation was simple and basic: the men slept on camp beds and made their own furniture in their spare time. North camp had showers; however, South camp did not, and therefore saltwater-lathering soap was provided for men to wash in the sea. The local wildlife intruded upon camp life, and whilst DDT was sprayed daily to protect the soldiers from malarial mosquitos, little could be done to prevent large land crabs from crawling into the soldiers’ tents at night. The men resorted to propping their beds up on jerry cans to reduce the likelihood of waking to find a crab nestled in their bedclothes. It was also a military offence to kill a land crab, as they were useful scavengers on the island. A veteran said that the local Fijians “… called [the crabs] Laro, and they ate them.” However, the soldiers did not, he reported. Otherwise, both soldiers and the Fijian camp community ate a diet of traditional British food and regional fruit and vegetables, including bananas and sweet potatoes. Food was served within the mess tent on compartmentalized metal trays, with depressed sections for main course and dessert. One veteran described the experience of mealtime to me, saying “… if you weren’t careful with your tray, your custard and gravy would escape and combine.” In addition to the mess tent, there was a church, an open-air cinema, and two “matronly” ladies of the Women’s Royal Voluntary Service who organized activities and games for the soldiers. Whilst the officers drank Grapple Slings, the young soldiers supplemented warm beer with moonshine brewed in gallon jars buried in the sand beneath their tents. The men went swimming, walking, and fishing, enjoying the idyllic tropical environment. However, this beautiful place was peppered with a light dusting of fallout after each test.
There was limited interaction between the soldiers and the Fijian community, although they performed general labor in camp, including emptying the Elsans (chemical toilets). Fijians were provided with multiple helpings of food whilst working, although whether this was due to undertaking more laborious work or to improve community relations is unclear. Some of the soldiers bought souvenirs and trinkets from the local community to take home to their families. There was a myth of the Islander Wife, the woman who fell in love with a soldier and left to marry him in the UK. Despite this, the communities remained separate.
The H-bombs were detonated every three months. The soldiers were sent outside and instructed to cover their eyes with their fists, and to face away from the blast. The health and safety officer said they would receive no more radiation than from an x-ray. Then business resumed as usual: the army cooks returned to preparing next meal, the aircraftsmen resumed vehicle maintenance. However, each nuclear blast produced an environmental legacy of radionuclides that were scattered across the land and sea by the wind.
Since gaining independence from the United Kingdom on 12 July 1979, Christmas Island is now known as the Republic of Kiribati. Changes have occurred on this tiny archipelago; exports of copra (dried coconut pulp) have grown, and it has become a destination for ecotourism. Whilst the atoll ecology is flourishing, radioactivity continues to permeate the environment. The Fijians and the young soldiers who lived and worked on Christmas Island cannot disregard their simultaneously mundane and unearthly experiences of paradise.
Appendix 3: Grapple Slings & Moonshine: Conversations with the men who tested atomic weapons on Kiritimati
European Research Council Toxic Expertise Research Group https://toxicnews.org/2016/08/03/grapple-slings-and-moonshine-conversations-with-the-men-who-tested-atomic-weapons-on-christmas-island/
Nuclear testing is often portrayed as a bombastic process, overshadowed by the devastating majesty of mushroom clouds and described in terms of annihilation or dramatic uncertainty. This is understandable, given the inherently destructive nature of nuclear weapons. However, my aim is not to sensationalise the British nuclear test series, but instead to provide a thought-provoking insight into the daily routines and experiences of the soldiers who travelled far from their families and homes to test the bomb.
Here, I share two personal narratives that describe some of the typical experiences of living within a military camp community, during British nuclear testing from 1952 to 1963. These particular communities and timescales are of interest to me due to being prior to the consolidation of the US-UK Mutual Defence Agreement. After 1963, much British nuclear testing was moved to Nevada, USA. However, prior to this, testing occurred on remote South Pacific British colonies. Therefore, some of the men toured Emu Field, across the desert of the Australian outback. Others visited Montebello Island near Australia; or Christmas Island, which is nestled within the Pacific Ocean. I have been told during conversations that “…people didn’t even travel to Spain” at this time, so I can imagine how exciting it must have been for the soldiers to have the opportunity to travel internationally. I personally still remember that precise moment when I stepped off an aeroplane for the first time, my own feet touching the burnished tarmac of Malaga airport. This was also the first chance for some of these men to leave their local communities. They travelled away from the tightly-knit social regulation of family and life-long friends, away from everything familiar, whilst jumbled up into regiments with a random assortment of other British soldiers. This the first time that many of these men would be able to define themselves on their own terms.
This piece explores two different personal accounts of travelling to Christmas Island. Whilst historically a colony, Christmas Island gained independence from the UK on 12th July 1979 and is now known as the Republic of Kiribati. It was the site of the Grapple test series from 1956 to 1958. In total, Operations Grapple X, Grapple Y and Grapple Z included nine nuclear detonations and enabled the UK to be recognised as the third nation to possess thermonuclear weapons. The first account describes the experiences of Ron, a member of the Royal Engineers regiment who had previously toured Germany before travelling by ship to Christmas Island on Boxing Day 1957, whereas the second account explores the experiences of Peter, a RAF Senior Aircraftsman (SAC) who flew for the first time on his first tour to Christmas Island in March 1958.
My first veteran, Ron, decided to join the army immediately after leaving grammar school. He told me “I left home in 1954, when I was sixteen. I’d lived away…on camp for a couple of years anyway”. He had completed his military training by the summer of 1957 and had experienced his first tour of Germany, before returning to his home unit in Rippon, Yorkshire. After travelling home for Christmas, he was redeployed to Christmas Island on Boxing Day in 1957. His experience was shared uniquely by his unit, as only the Royal Engineers travelled en-masse by boat. “The whole unit went on a specially chartered train to Southampton, all thousand of us, then onto the boat and off we went…”. The young soldiers shared facilities in the hull of ship, sleeping in bunks that were three to four beds high. “The ship got out of Southampton and then trundled off into Atlantic. Most people were seasick for the first week, until reaching the Bay of Biscay. I was lucky though, as I was on the top bunk and wasn’t sea sick. The first week there was no queue for breakfast because of the seasickness. It was great until people started to recover, then you can imagine the queues”. I was told “There was tombola to keep us entertained and guard duties to keep us busy…We’d practice shooting on deck, throwing floating things over the side to aim at…”. The ship refuelled at Curacao, then travelled through the Panama Canal, with a stop-off at Panama City. Ron revealed a little about it. “We had a night out in Panama, we hit the bars and then the strip clubs…”. Hangovers must have been nursed as ship left the docks, and began venture across the Pacific Ocean on route to its final destination.
Initially unbeknownst to Ron, this ship also had an additional cargo of veterans wives and families. He told me a little more about this, and he said “Much of it was a publicity stunt. The boat went out with us all, and returned with the soldiers who were currently there. They were able to meet up with their families on the ship, and to have a cruise home together which was paid for by the MOD. I didn’t see many of them, I think we were kept separately”. Whether it was a generous gesture, or a way to publically humanise the soldiers and separate them from their work, it must have been incredible for these men to have had such an unanticipated reunion. The regiment arrived in January 1958 after three weeks of travelling. The boat had to anchor offshore, and soldiers were shipped onto the island by landing craft.
Ron described the soldier’s accommodation on the island in no uncertain terms “The tents were very primitive. We slept on camp beds, with metal legs to clip in, about 6 to 8 inches off the ground. The tents were big, with at least ten people in each tent. We were provided better beds later on…It was the way things worked, occasionally the supplies arrived before the soldiers”. He shared a disconcerting tale about the local wildlife. Large land crabs were abundant on Christmas Island, and “…they crawled into the tent and crawled over you at night”. His solution to this problem was to prop up his bed on jerry cans at night and to hope that he didn’t roll out in his sleep. We talked about day-to-day life on camp, and he said that whilst the main northern camp had washing facilities, the southern camp did not. The soldiers were provided with salt-water lathering soap and instructed to wash in the sea. He said “Think of all those naked young men running into the sea, it was quite a sight!”. I was momentarily lost for words, before bursting into laughter and jokingly asking for photographic evidence.
There was a cinema, a mess and a church. He was proud to tell me that there were two women from the Women’s Royal Voluntary Service (WRVS) who were permanent residents on camp. They had their own accommodation hut and were described by him as “matronly types”. Ron didn’t have much to do with the local population, as the locals lived mainly around the port. We talked leaving the island. He said that he only left twice during his time there, and told me about an unusual example of camp solidarity when he attended a funeral, a burial at sea away from the island. He was required to participate and I asked him if he knew anything about the deceased. He told me “I don’t know why he died, I just had to do the honours”. No questions were asked. The second time Ron left the island was more cheerful, as all the soldiers were provided with a holiday, and those on Christmas Island were sent to Hawaii. He therefore left Christmas Island for a week of relaxation, but ended up staying for an extra week because the plane “conked out”. This plane was also used to pick up supplies, such as fresh fruit and vegetables. When I asked about the food on camp, he described it as “normal” for the time. I told him I was interested in his day-to-day life, but somehow our conversation diverged. Instead, we talked about managing risks to health, and he described the white powdery anti-malaria tablets that were prescribed with each meal. He also told me that the entire camp was “zapped” daily by an aeroplane spraying DDT to kill mosquitos. He said it was commonplace at the time, but he was concerned about the effects of inhaling biocide.
I wanted to know how Ron spent his free time, and we talked about how the lack of local travel restrictions on the island. “I used to go swimming, go walking, I’d borrow a 4×4 and take off to a lagoon in the middle of the island”. He told me that learnt to drive without a licence, whilst working for a scientist from Aldermaston. He would tow and set up the generators for the scientist’s cameras. There also were no petrol stations, just jerry cans of petrol which were emptied and left on the side of the road, and were later re-filled by another soldier. Unsurprisingly, the soldier’s work and life seem deeply intertwined.
The last thing we spoke about was family. I asked him if he missed his parents whilst he was on tour, but he’d previously left home at sixteen. Letters were written to the soldier’s families by the commanding officer. He said “these letters explained where we were and what we were doing, for instance, constructing buildings or repairing roads. My mother kept mine – I discovered them in her home after she passed away. I still have them”. Ron also wrote letters to his mother himself, and posted some more unusual souvenirs of his experience. “I used to post coconut shells back to England – you’d just write the address on the shell”. I asked for his final thoughts on the experience at the time, and he said to me “You can’t imagine…it was so exciting”. However, in the years that have accumulated since atomic testing, his perspective has changed. He worries about the health of his contemporaries and the impact upon their families. He has requested his own military medical records with little success. Whilst he is healthy, he worries about the availability of information, and wonders whether this material has been intentionally misplaced rather than lost. I thanked Ron for sharing his experiences with me and wished him well.
My second veteran, Peter, was called up for National Service. His first posting was in 1957, to RAF Stanbridge for a year of training before travelling to Christmas Island. RAF Stanbridge was an attachment of Bletchley Park during the Cold War. He described Stanbridge to me as “…behind a fence, everything (the facilities for the soldiers) was outside, and the RAF police were armed, which was unusual in those days – Even the police didn’t know what we did”. It sounds like an interesting but formidable environment. Peter told me a story about his trip for a medical before travelling to Christmas Island. He was told to report to RAF Wroughton hospital, to have a small scar examined from surgery during 1949. He told me that he had been “on sick” a couple of times previously, due to pain from this scar, so this seemed reasonable. However, he described his surprise at being retained for medical monitoring. “I went, and I was in there for four days – they didn’t let me shave and then four days later they discharged me. I received a medical before leaving. They monitored my blood pressure, pulse, temperature, took a couple of blood samples”. Peter continued to tell me about his first experience of travelling, “I had never flown before I travelled to Christmas Island. I was notified about a week in advance. I was told to go to London airport with my coat and kit bag… we travelled with everything. There were men with overcoats and gloves travelling to a tropical island. Can you imagine!”. He said that he didn’t know anyone when he arrived at the airport, but that he quickly made friends with some of the other servicemen on the flight. He flew with British Overseas Airways Corporation (BOAC), the forerunner of British Airways. The flight was palatial, as BOAC was the “posh airline of the day, proper china and glass and all that – none of the plastic stuff”. Peter flew from London to New York, then from San Francisco and beyond with PanAm (Pan-American Airlines). When he arrived in San Francisco he was given the option of either remaining in the airport, or taking a guided coach tour of the city with the other soldiers. He recalled that it was a hot day and that neither choice sounded appealing –instead, he made the decision to sneak out of the airport with another soldier, after the other men had left for the coach tour. They hadn’t got far before they were stopped by local policemen. They asked to go somewhere nice, and were given a lift to a small town near the airport called San Bruno. Peter told me “We walked into the bar and felt like stars for the day. A couple of expats came up to meet us, and there were some incredible stories. We got quite drunk. When we left, we called a taxi back to the airport, and discovered that our taxi had already been paid for. Everyone else returned from the coach trip looking glum, so we had to be quiet about our adventure”. I asked him how he would describe the travelling experience, and he said “It was an adventure, a luxury holiday across the world”.
Upon arrival on Christmas Island, Peter initially lived in a transit tent, before being moved to the JLC line, which he described as being the nerve centre of the island. He shared a three berth tent, specifying that there were no two berths due to the historical prohibition of homosexuality. His environment was spartan “You were given a camp bed, which was made of springs with material stretched across it. We had to keep them off the ground, otherwise you’d wake up in the night with a land crab on your chest – they sought out the warmth of your body”. It was a military offence to deliberately kill a land crab, primarily because they scavenged rubbish, but also because thousands of bluebottles bred within the shells of the dead ones. I was rapt as Peter continued to describe them as “…big old things. They could open a coconut – they would get their claws into the indents at the top and get them open. People didn’t like them, but they did you no harm unless you annoyed them, and then they would spit at you”. My eyes widened in surprise at the spitting crabs, and he chuckled at my reaction, before continuing to say “There’s a lot you don’t know! The Fijians called them Laro and they ate them – we didn’t though”. Peter attended an induction at the open-air cinema when he arrived on the island. He said that for soldiers, radiation was just another piece of jargon. The health and safety officer said to them that they would receive no more radiation than from an x-ray, during their time on Christmas Island. They were told to face away from any detonations, and to cover their eyes with the palms of their hands. During this briefing, the soldiers were also warned to protect themselves from sunburn and sunstroke by wearing regulation scarves, hats and sunglasses. Sunburn was classified as a “self-inflicted injury” by the forces. However, on return from his briefing, Peter was informed by his own duty officer that wearing his sunglasses would weaken his eyes. Peter felt obliged to listen to him, despite the conflict of available information.
Peter celebrated his twentieth birthday one week after arrival, and his description of this provided an interesting insight into camp social culture. He told me “there were no spirits available for us lads, only the officers had spirits, so we got drunk on warm tinned Guinness and brandy. The Guinness was out-of-date and the refrigeration system had broken”. There was a disparity between the experiences of the soldiers and the officers. The senior ranks relaxed and drunk Tom Collins and Grapple Sling cocktails in the officers’ facilities, delicate combinations of gin or whisky with tonic water, lemon and sugar syrup. Whilst the officers enjoyed civilised socials, the troops were attempting to make their own potent moonshine to supplement their “tinnies”, which was brewed in gallon jars that were covertly buried in the sand beneath their tents.
There was a designated mess tent, where the soldiers ate from utilitarian metal trays with compartments for each type of food. Peter recalled that “if you weren’t careful with your tray, your custard and gravy would escape their respective compartments and combine. The food was fairly normal, but we did have to pick steam flies (cockroaches) from the bread sometimes. It was the first time I ate sweet potatoes, every day was the same, you had breakfast, dinner and lunch”. He told me that whilst the soldiers had one portion per meal, the Fijian community who were working on camp could return multiple times for further helpings of food. I wondered if this was because their work was more arduous, or if it was an attempt to improve local community relations. The Fijian community were general labourers, emptying the Elsans (chemical toilets), which Peter described as “pretty revolting”. Whilst the soldiers enjoyed meeting others at the NAFFI, Peter told me that you “stuck to your own lot” and didn’t fraternise with the locals.
We talked about his journey home on the Captain Cook. He described the ship as a “a rust bucket, I think it was the last trip it ever did…”. He also experienced a night in Christabel, Panama. “It was rough…a Caribbean-type port and all the locals were skint. They latched onto us for anything they could get. We had a few beers, and a few blokes got drunk and ended up in places they shouldn’t have”. Following this, the ships lined up to travel through the Panama Canal. The merchant ships had organised for the nuclear veteran’s ship to travel first and lead the way through the canal, as a mark of respect to the soldiers. The final stop was Curacao. Peter said that “It (the ship) was only for service-people, but we were all from different parts of the island…Whilst travelling, we talked and discovered that different people in different places wore different things”. He pauses to contemplate whether this was because of differences in radiation protection need, or due to experimentation by the British government. A big question, and not one that I felt qualified to try to answer. The ship docked in Southampton on return. Peter said “My old man had a factory there so I could dump my stuff at his place. My officer told me to find myself some lodgings and not to come back in uniform. I had to find civvy digs (civilian housing), it was like working for the government. Before Peter left, I asked him how he felt about being a nuclear test veteran, and he told me “I felt privileged to see something that no one else had, it was a unique experience”.
Both Peter and Ron’s stories of time spent Christmas Island share parallels, but each also has a uniqueness which has been determined by that man’s own personal history and positionality. What is recalled and what is forgotten, what is significant or trivial to each individual. It has been a privilege to talk to both men, and I’m looking forward to approaching their discourse with an academic gaze as my research progresses.
Appendix 4: Keep the home fires burning: Rekindling the Flame with the French and British nuclear test veterans
I explore the lives of international nuclear communities, discovering the human and cultural experiences and impacts of ionising radiation to individuals and societies. My current major research project with the University of Southampton is called Nuclear Families and provides an in-depth investigation into the lives of the British nuclear test veterans and their families.
As part of this project, I was invited to document the first Anglo-French Rekindling of the Flame above the Tomb of the Unknown Soldier under the Arc de Triomphe on July 2nd 2016. The flame was first lit on November 23rd 1923, and has since been rekindled at 6.30pm each day by a variety of different French military and veteran communities. However, there has been comparatively little British rekindling with only the Queen and Prime Ministers Winston Churchill, Antony Eden, Howard McMillan and Tony Blair having gained this unique honour.
The ceremony was undertaken by British Nuclear Test Veterans Association Chairman and Maralinga nuclear test veteran Mr Jeffery Liddiatt, in conjunction with Mr Jean-Luc Sans who is president of AVEN, the French atomic veterans association. It was an incredibly poignant and commemorative moment when they lent together to reignite the eternal flame, and an exceptional demonstration of several years of solidarity that have existed between the French and British nuclear communities. There were veteran representatives present in full military regalia, not only from the British Christmas Island and Maralinga tests, but also from the French Algerian and Polynesian tests.
This year has been significant for the British nuclear test veterans, who have gained £1 million research and care funding in March, and were granted Consultative Status by the United Nations in April this year. It seems that the achievements of the men who worked on our nuclear deterrent during the Cold War are finally gaining international recognition.
Appendix 5: Participant Information Sheet
Participant Information Sheet
Study Title: Nuclear Families
Researcher: Becky Alexis Martin Ethics number: 19266
Please read this information carefully before deciding to take part in this research. If you are happy to participate you will be asked to sign a consent form.
What is the research about?
The Nuclear Families project is a human and social sciences research project which explores the lived experiences of the families of UK nuclear test veterans. Becky Alexis Martin is a Research Fellow in Human Geography at the University of Southampton, and is the project lead.
The purpose of this work is to discover more about the psychosocial effects of being related to being a nuclear test veteran and to explore the impacts of this upon wellbeing, welfare, mental health, relationship dynamics and the community as a whole. Funding for this work has been provided from an NCCF grant via the British Nuclear Test Veterans Association.
Why have I been chosen?
You have been selected for this study as an individual who is related to a British nuclear test veteran.
What will happen to me if I take part?
If you choose to take part, you will participate in a semi-structured interview, which will document your lived experiences as a family member of a nuclear test veteran. The interview will take a maximum of 90 minutes and will be completed in person.
There will also be the opportunity to participate in further interview-based and ethnographic studies, on a self-selecting basis.
Are there any benefits in my taking part?
There is no individual benefit to your taking part. However, there will be significant development of current knowledge of the collective experiences of the families of nuclear test veterans.
Are there any risks involved?
Some questions may broach sensitive topics, relating to your personal health and wellbeing. You are welcome to decline to answer, or to curtail the interview at any point in time and without explanation.
Will my participation be confidential?
Your participation will be confidential as possible, and individual interview data will be anonymised. All data will be collected and stored in compliance with the Data Protection Act and University Policy, data coded and stored on a password protected computer.
Any material that is published as a consequence of this work will be anonymised, however individual responses related to personal experience may still include some identifying characteristics.
What happens if I change my mind?
You are welcome to withdraw from the study at any time, with no consequence to yourself or others.
What happens if something goes wrong?
Please contact the Head of Research Governance at the University of Southampton if you have any concerns or complaints (02380 595058, rgoinfo@soton.ac.uk).
Where can I get more information?
Please do not hesitate to contact Becky Alexis Martin at becky.martin@soton.ac.uk or 07885 608573 for further information or questions about this project.
Appendix 6: Participant Invitation
Population, Health and Wellbeing (PHeW)
44/2101: Human and Social Sciences
University of Southampton
Highfield Campus
Hampshire, UK
SO17 1BJ
(02380) 592205
(07885) 608573
Dear Study Participant,
Firstly, I want to thank you for getting in touch with the Nuclear Families project team at the University of Southampton.
Nuclear Families is a new NCCF-funded project which is designed to gain a deeper understanding of your lived experiences. We have a team of experts within the human and social sciences who will be exploring what it means to be part of the nuclear community by learning more about your experiences and perceptions of welfare, wellbeing, mental health, disability, family, society, stigma and risk.
This is a self-selecting study, therefore anyone who is part of the nuclear community is welcome to participate. Mothers, wives, daughters, sons, grandchildren – You don’t need to be a member of the BNTVA or any other similar organisation, and we would encourage you to share our study details with your friends and relatives who may be interested.
We will be using variety of different methods for this work including interview, group study, diary-keeping and observation techniques. The first stage of the study is a confidential in-depth interview with you. We have comprehensive ethical approval from the University of Southampton to start work now, so we are ready when you are. We can visit you, or alternatively you can visit us at the University of Southampton to take part. Please get in touch with us by email, phone or post to schedule your meeting.
Looking forward to hearing from you!
All the best,
Becky Alexis-Martin
Principal Investigator: Nuclear Families
Research Fellow in Nuclear Geographies, PHeW Research Group, University of Southampton.
Appendix 7: Semi-Structured Interview and Questionnaire
This interview is part of a project funded by the NCCF, that is being used to understand the experiences of the family members of British Nuclear Test Veterans. The responses are anonymised, unless you choose to give us your name because you ask to be contacted as the study progresses.
- Gender
☐ Male☐ Female ☐Prefer not to say
- Age
☐ 16-25☐ 26-35☐36-45☐46-55☐56-65☐66+
- Marital Status
Could you tell me a little about your marital status?
☐ Single/Never married ☐ Married or domestic partnership ☐ Widowed ☐ Divorced ☐ Separated ☐ Cohabiting ☐ Other
(Home)
- Could you tell me a little about your immediate family, and what they are like?
- Do you know which nuclear testing events you/your relative was a participant in?
- What role did you/your relative have in the testing (was it scientific or military)?
- Was there any discussion of their experiences of nuclear testing, within the home?
- If so, how did this make you feel?
- When did these conversations occur?
- If there was not discussion of this, how did you learn about their experiences, and from whom?
- Were there any changes to your home life, after your family member returned from nuclear testing?
- If there were changes, how did these changes affect you?
- What is the current status of your relationship with your nuclear test veteran family member?
- How would you describe your current relationships with partners and/or friends?
- Do you feel that these relationships have been influenced by your experience of family, and if so, in what way?
(Disability)
- Could you tell me a little bit about your health?
- Do you consider yourself to have a disability?
- What sort of disability do you have?
- Could you tell me a little more about this please?
- What impact does this have upon your day-to-day life?
- Has this affected your capacity to work?
- Has this affected your capacity to socialise?
- Do you feel as though your condition is associated with your nuclear test veteran heritage, in some way?
- Could you please tell me more about this?
- Have you experienced any preconceptions or stigma as a result of any health issues?
- Has anyone in your immediate family, experienced any form of stigma or preconceptions as a result of any health issues?
(Mental Health)
- If you don’t mind, would you be OK to discuss mental health?
- Do you have any of the following conditions?
` PTSD
Anxiety
Depression
Panic attacks
Other mental health symptoms (specify if possible)
- Are you currently receiving treatment for your condition?
- Is there anyone else in your family who experiences similar symptoms to yourself?
- Are they a nuclear test veteran?
- Are you aware of any specific conditions that your relative experienced?
- Do you believe these were related to their experiences as a nuclear test veteran?
- Similarly are you aware of any experiences of mental health within rest of your immediate family?
- Are you aware of any specific conditions which were experienced?
- Do you believe these were related to having a nuclear test veteran as a family member?
(Welfare and Wellbeing)
- Do you currently receive government financial assistance to help with any health conditions?
- What level of financal assistance do you receive?
- Is this a sufficient level of assistance?
- Are you a smoker?
- How many cigarettes do you smoke?
☐ 1-5 ☐ 6-10☐ 11-15 ☐ 16-20 ☐ 20+
- Do you drink alcohol?
- How many units per week (one unit is equivalent to one spirit measure, ½ pint of beer or lager, 1 alcopop, or a small glass of wine – bring infographic)?
☐ 1-3 ☐ 4-6☐ 7-9 ☐ 10-12 ☐ 13-15 ☐ 16+
- Do you have any care responsibilities, and for whom?
- How would you describe your day-to-day wellbeing (1 is poor and 5 is high)?
1 2 3 4 5
- Why did you select this criteria?
(Risk and support)
- Have you personally experienced any distress or concern, due to worries about radiation exposure?
- Have you experienced any distress or concern, due to worries about the hereditary effects of radiation exposure?
- Could you tell me more about this?
- Do you know of anyone else in your family who has experienced distress or concern, due to worries about radiation exposure or its hereditary effects?
- Which family members?
- In way ways do you think it has affected them?
- What resources do you access to help to understand risk?
- In what way do these resources help you?
- What support have you found most useful for improving your understanding, as a family member of a nuclear test veteran?
- Why has this been helpful to you?
- Is there anything else that you would like to tell us about your own experiences as a family member of a nuclear test veteran?
THANK YOU FOR YOUR TIME.
Appendix 8: Consent Form
CONSENT FORM
Study title: Nuclear Families
Researcher name: Becky Alexis Martin
Ethics reference: 19266
Please initial the box(es) if you agree with the statement(s):





Data Protection
I understand that information collected about me during my participation in this study will be stored on a password protected computer and that this information will only be used for the purpose of this study.
Name of participant (print name)……………………………………………………
Signature of participant……………………………………………………………..
Date…………………………………………………………………………………
Appendix 9: Ethics sub-committee application form
1. Name(s): Becky Alexis-Martin
2. Current Position Research Fellow in Human Geography
3. Contact Details:
Division/School Geography and Environment
Email Becky.martin@soton.ac.uk
Phone 07885 608573
4. Is your study being conducted as part of an education qualification?
5. If Yes, please give the name of your supervisor
6. Title of your project:
Nuclear Families
7. Briefly describe the rationale, study aims and the relevant research questions of your study
It is exactly twenty years since the Comprehensive Nuclear Test Ban Treaty (CNTBT) in 1996, a treaty which prohibited all explosive nuclear testing for both civilian and military purposes. Whilst the lives of the nuclear test veterans have been rigorously explored within the quantitative sciences, there has been limited prior academic research of the nuclear veteran family community within the social science domain.
A single relevant USA small-scale cohort study was produced 25 years ago, which examined the responses of atomic veterans and their families to radiation exposure by an in-depth interview approach (Murphy et.al. 1990). However the culture and society of the USA is not comparable to the British experience; and the scope and depth of this study is limited. Therefore, the Nuclear Families study aim is to develop a comprehensive understanding of the lived experiences of the families of the nuclear test veterans, and to discern how this has impacted upon their wellbeing and life outcomes.
The Nuclear Families project will provide a contemporary approach to understand the lives of the families of British nuclear test veterans. The project will combine methodologies across the social and human sciences to explore this unique group. A new review of relevant literature will provide objective historical and social context to the study. A series of semi-structured interviews will be implemented to tackle themes pertaining to well-being, welfare, family dynamics, mental health, disability and stigma. Focus groups will be conducted to gain insights into group dynamics, thoughts and feelings, within the context of the cohort gaze. Finally, an ethnographic approach will provide a uniquely subjective overt participant observation of the family experience, in contrast to the other research methods employed by this study. This programme of research will also be complemented by basic demographic data, which will contextualise the experiences of the cohort.
However, the Nuclear Families project is not just an opportunity to learn from and to understand the lives and the experiences of the families of nuclear test veterans, but also a chance to inform the direction of policy for future support to these families.
8. Describe the design of your study
The study is implemented to explore perceptions of well-being, welfare, family dynamics, mental health, disability and stigma within the nuclear family cohort. The study is designed to include phases which will enable review and the further refinement of subsequent work, which will hopefully create an element of concurrent validity as the project progresses. A phenomenological approach is required, as the study is focused upon the interpretation and perceptions of impact of being a family member of a nuclear test veteran, rather than the practicalities of actually being exposed to ionising radiation.
An inductive approach will be taken, as current background information is too limited to create effective deductive hypothesises within this domain. A case study approach will be adopted across the project, and qualitative information will be self-reported by the participants throughout its duration. Interview-based and focus group methodologies will be implemented, and differences between participant reporting across approaches within the same theme will be analysed for elements of bias and performativity.
An ethnographic overt participant observation methodology will also be implemented for a select number of participants, to gain insight into their day-to-day lived experience. These participants will be self-selecting, specifically recruited on the basis of their attendance of the BNTVA annual AGM conference and willingness to participate in interview and focus group work.
This study will utilise participant observation as one of its research methods. Participant observation has the benefit of studying research participants in a natural and uncontrolled setting. This would provide an insight into the day-to-day lives of the families of nuclear test veterans, and would allow for the collection of data regarding the interactions between research participants. Participant observation would be performed overtly with select participants within the cohort over varying periods of time. The ethnographic study will be conducted with individual members of the cohort in the run up to a BNTVA event, with the event being the final aspect of the participant observation. Two participant observations would be run simultaneously with separate participants and researchers with an aim to correlate the results. The participant observations would be followed up with a final semi-structured interview to review the participant’s thoughts and feelings towards the experience.
This programme of research will also be complemented by the collection of basic demographic data during interviews and focus groups. Interviews, focus groups and overt participant observation will be audio-recorded; and consent to recording will be audio-registered. In a scenario where audio-recording is not explicitly agreed to, the interview will continue without recording, and will be registered through a greater focus on note-taking.
9. Who are the research participants?
The research participants are the family members of British nuclear test veterans.
10. If you are going to analyse secondary data, from where are you obtaining it?
No secondary data will be included within this study, beyond relevant academic review papers and associated material within the public domain.
11. If you are collecting primary data, how will you identify and approach the participants to recruit them to your study?
Please upload a copy of the information sheet if you are using one – or if you are not using one please explain why.
There is an existing cohort of study participants, who are members of the British Nuclear Test Veterans Association and Fallout. These organisations exist to support the veterans and their families, and participants will be identified and approached for recruitment through a targeted strategy of project promotion and contact by both the study, and the relevant organisations.
In addition to this, future participants within and beyond the scope of these organisations will have the opportunity to provide their details for recruitment at BNTVA events, including the AGM on 21st May 2016.
12. Will participants be taking part in your study without their knowledge and consent at the time (e.g. covert observation of people)? If yes, please explain why this is necessary.
No, all work will be completed with the knowledge and consent of participants. There will be no covert observations made.
13. If you answered ‘no’ to question 13, how will you obtain the consent of participants?
Please upload a copy of the consent form if you are using one – or if you are not using one please explain why.
Consent will be obtained through the use of a consent form supplied to the participants prior to interview alongside a participant information sheet. Participants we have the right to withdraw consent at any time during the study.
14. Is there any reason to believe participants may not be able to give full informed consent? If yes, what steps do you propose to take to safeguard their interests?
The recruitment strategy will be targeted to ensure that individuals who may not be able to provide full informed consent are not included. I will ensure that prospective participants are over 18 prior to engaging them in the research process. Participants will be approached through the BNTVA and web forums, and as stated above, the recruitment strategy will be targeted to ensure that individuals who may not be able to provide full informed consent are not included, and as a result participants will be able to make their own decision regarding participation.
15. If participants are under the responsibility or care of others (such as parents/carers, teachers or medical staff) what plans do you have to obtain permission to approach the participants to take part in the study?
N/A
16. Describe what participation in your study will involve for study participants. Please attach copies of any questionnaires and/or interview schedules and/or observation topic list to be used
Participants are family members of nuclear veterans of adult age and will be recruited through BNTVA events and literature, and subsequently through snowball sampling. Participants will be approached personally at BNTVA events, and recruited by the confidential collection of contact information, which will be stored securely on a password-protected computer following collection. Participants will also be recruited by relevant online and paper media calls for participation, to enable individuals to self-select and get in touch.
Study participants will initially partake in semi-structured interviews, which will be then followed up by their participation in relevant focus groups. These two approaches will document the lived experiences of participants as a family member of a British nuclear test veteran. The semi-structured interviews will take a maximum of 90 minutes, focus groups a maximum of two hours.
There will be opportunity for participants to be involved in further work on a self-selecting and researcher-selecting basis, specifically a small-scale study of 3-5 individuals, which will utilise overt participant observation to create ethnography of the lived experience of these 3-5 veteran family members, and their family and daily life, for five days before in preparation for, and during the BNTVA AGM 2017. The participant observation aspect of this will be negotiated on a case-by-case basis with the relevant participants who express interest in involvement, at the time of study sign-up.
To support this, a semi-structured interview, focus group, and overt objective participant study design have been included, in conjunction with corresponding participant information sheets for each activity.
17. How will you make it clear to participants that they may withdraw consent to participate at any point during the research without penalty?
All documentation provided will clarify that consent to participate may be withdrawn at any point. All interviewers will be required to explain this verbally prior to initiating work, and after completion, to ensure that consent to withdraw is understood and accepted by participants, and that participation is completely voluntary.
18. Detail any possible distress, discomfort, inconvenience or other adverse effects the participants may experience, including after the study, and you will deal with this.
The interviews are not expected to be emotionally distressing or uncomfortable. However, since the topic of the study might be sensitive, a possible adverse effect may arise when a participant does not wish to respond to one or more of the questions asked.
Within this scenario, the researcher will simply move onto the next topic and related questions. At no point will a project participant be made to feel pressured to answer questions. Participants will be given the option to withdraw their consent as a study participant at any time, and will have the capacity to discuss the study further with the researcher, and will be provided with documentation that includes the contact details of relevant helpful organisations with counselling capacity, including the BNTVA and The Samaritans.
The BNTVA have been consulted on this, and have agreed to consent to the provision of counselling by a trained counsellor who supports their organisation, to support this study should any difficulties occur, with or without relevance to specific study topics.
19. How will you maintain participant anonymity and confidentiality in collecting, analysing and writing up your data?
It should firstly be noted that it is impossible to completely safeguard anonymity, but all possible methods will be implemented to ensure least risk. Individually collected data will be coded upon collection, analysed under code and written up without personally identifying features, such as name or address. Any material that is published as a consequence of this work will be anonymised, however individual responses related to personal experience may still include some identifying characteristics, as this is a case study approach. If this issue arises, then contact will be maintained with participants to ensure that levels of disclosure are acceptable.
20. How will you store your data securely during and after the study?
The University of Southampton has a Research Data Management Policy, including for data retention. The Policy can be consulted at http://www.calendar.soton.ac.uk/sectionIV/research-data-management.html
There are several necessary steps to be followed to ensure and maintain data-security and data-protection during fieldwork:
At the earliest opportunity the researcher will separate the storage of the consent forms from the digital media (voice recordings, photographs etc), which will be then transferred to a secure university computer, following which, everything will be deleted from the portable devices.
All personally identifiable material will be removed and replaced with a randomly generated code or pseudonym, within the interview schedule and files, for example. This randomly generated code will be the only thing kept with data for identification purposes. The random linkage code personal details will then be securely recorded within an encrypted and password protected file on a different computer where no research data is stored, against the names of the participants. This will prevent access to both data and linkage codes in the event an incident, such as the theft of a laptop for example.
For backup and security purposes, the research data will be uploaded onto a hard drive, which will be based in the office of the primary investigator on this research project, and kept in a locked desk. An online back-up will also be created automatically on the servers of the University (in alignment with the University’s IT team). During the research in the field, recordings of the interviews and observations will be kept upon a voice and/or camera, which will be kept with the researcher at all times.
The data will be handled confidentially, stored and retained upon password-protected computers in compliance with University data policies for a period of 10 years, after which time it will erased or otherwise disposed of in a secure manner. It is important to store data securely both during and after the study. Data relating to this study will be handled confidentially and stored retained in accordance with the principles of data protection outlined in University of Southampton’s Research Data Management Policy for a period of 10 years, after which time it will be erased or otherwise disposed of in a secure manner.
21. Describe any plans you have for feeding back the findings of the study to participants.
The findings of the study will be fed back to participants through the BNTVA magazine. Additionally, an open end-of-project conference will provide the researchers with the opportunity to showcase their work to the cohort, a copy of the final project report will also be offered to all participants.
22. What are the main ethical issues raised by your research and how do you intend to manage these?
The key ethical issue of this research is the study of a potentially vulnerable population. This will be managed through making it clear to participants that consent can be withdrawn at any time, that participation may be ceased at any time and there is no obligation to answer any question if the participant does not feel comfortable in doing so.
23. Please outline any other information you feel may be relevant to this submission.
Please note the expected starting date of research is 19th May 2016.
I have sought to submit this Ethics Sub-committee Application Form before the start of this study, as the BNTVA and Fallout (families group) annual AGM 2016 is occurring on 20th-23rd May. This would provide a unique and significant opportunity to have conversations with individuals that may lead to development of our understanding of the wellbeing of the families of nuclear test veterans and is likely to be significant to the further development of this project.
Appendix 10: Further Outputs – Talks and Presentations
Eight talks have been given on Nuclear Families research. This includes six academic talks, including four academic peer-reviewed conference events, where abstracts were submitted. Selected abstracts are included.
- Nuclear Families – Nuclear Geographies. Manchester Metropolitan University. 30th October 2018

- Nuclear Families. All Tests Reunion. Weston Super Mare. 19th-22nd October 2018.

- Nuclear Families – Nuclear Geographies. Royal Geographical Society. 19th October 2018

- Nuclear Families. Toxic Expertise. European Research Council. 16th April 2018.
- It Runs in the Family: Understanding Reproductive Decision-making by the Daughters of Nuclear Test Veterans – Interdisciplinary Social Sciences, Japan. 26th – 28th July 2017.
Becky Alexis-Martin, Geography and Environment, University of Southampton, UK; Mwenza Blell, Sociology, University of Cambridge, UK
At the dawn of the Cold War, the UK undertook a series of nuclear weapon tests in Australia and the South Pacific. Whilst the tests situated the UK as a significant geopolitical power, some significant physical and mental health challenges later emerged for the men who tested these weapons. These men are known as the nuclear test veterans. However, there is complexity to the nuclear test veteran experience of health and wellbeing, due to the inherently nebulous relationship between humans and ionising radiation. This has resulted in contested and unattributed diagnoses that have no clear biopolitical endpoint. For the first time, we examine the perceptions and experiences of care within the nuclear test veteran family community. Individual and group interview accounts by both veterans and their families, have allowed for their lived experiences of both caring and receiving care to be explored. This study identifies the previously concealed dynamic of informal hidden care and self-care within this community. We proceed to investigate the particular complexities and tactics that emerge along the journey to care. We therefore explore how experiences of care have shaped the nuclear test veteran’s struggle to find health and wellbeing, despite adversity.
- Family Values: Psychosocial wellbeing and perception of risk within the Nuclear Test Veteran Community– Nuclear Geographies – Royal Geographical Society. 1st September 2016.
Nuclear Test Veterans have been impacted by an uncertainty of perception of risk of radiation exposure, due to the covert nature of their work during the Cold War. Whilst there has been some exploration of the psycho-social effects of perceived radiation exposure to radiation emergency survivors (Martin, 2015), this is currently uncharted territory within the domain of the Nuclear Test Veterans and their families. This paper examines the possibility of psycho-social effects to families of Nuclear Test Veterans, from the perspective of mental health and perception of risk. A combination of qualitative and quantitative approaches is applied to understand and identify existing mental health diversity and mental health themes within the descendant community. An interview-based methodology is implemented identify any cross-generational constructs of radiation risk may have impacted upon the behaviours and attitudes of descending generations. By this approach, the study presents novel insights into intergenerational attitudes across an exceptionally unique and important cohort.
- Nuclear Families and Gentleman Activists – Colorado State University. October 2016.

- Nuclear Families. BNTVA AGM. 20th-22nd May 2016.


Glossary
Acute radiation syndrome (ARS): The onset, within hours of high dose whole body irradiation, of nausea and vomiting followed by destruction and diminished (or absent) replacement of essential blood cells resulting in vulnerability to serious infection and bleeding; recovery is possible but with increasing doses these effects are more severe and death is more likely.
Alpha particle: A particle consisting of two protons plus two neutrons; emitted by a radionuclide.
Background radiation: Ionising radiation from naturally occurring radionuclides both in the environment (from soil, rock and building materials and from space – cosmic radiation) and in the body.
Beta particle: An electron emitted by the nucleus of a radionuclide. The electric charge may be positive, in which case the beta particle is called a positron.
British nuclear test veteran: A veteran of the British early Cold War nuclear weapon test series in Australia and the South Pacific.
British nuclear test veteran’s association (BNTVA): A charitable organisation for the support of British nuclear test veterans.
Contamination: The suspension in air or deposition of radionuclides upon, or in, the ground, water and other surfaces, and personnel and equipment
External contamination: Of a person or equipment – deposition, general or localised, of radionuclides upon all or any of clothing, hair, skin and/or equipment
Internal contamination: Of a person – deposition within the body, usually by inspiration, by ingestion or sometimes through penetration of (usually broken) skin by radionuclides which will then irradiate the cells of surrounding body tissues.
Cosmic rays: High-energy ionising radiation from outer space.
Decay: The process of spontaneous transformation of a radionuclide; the decrease in the activity of a radioactive substance.
Dose: The amount of ionising radiation received, as deduced from the energy absorbed from an external radiation source
Absorbed dose: Quantity of energy imparted by ionising radiation to unit mass of matter such as tissue. Unit is the gray, symbol Gy. 1Gy = 1 joule per kilogram
Equivalent dose: The quantity obtained by multiplying the absorbed dose by a factor to allow for the different effectiveness of the various ionising radiations in causing harm to tissue. Unit is the sievert, symbol Sv
Effective dose: The quantity obtained by multiplying the equivalent dose to various tissues and organs by a weighting factor appropriate to each and summing the products. Unit is the sievert, symbol Sv.
Dosemeter: A small device worn on the person to measure absorbed energy and from which a record of Absorbed Dose may be obtained.
Dosimetry: The estimating, recording and maintaining of records of dose.
Emitter: A radionuclide decays by emission of certain radioactive particles and/or electromagnetic radiation. A particular radionuclide may be described as an alpha or beta or beta/gamma emitter.
Fallout: The transfer of radionuclides produced by nuclear weapons from the atmosphere to earth; the material transferred.
Fission products: The two, invariably radioactive, fragments remaining after an atom has been split (undergone fission).
Fission-line: A magazine produced by British nuclear test veterans.
Gamma ray: A discrete quantity of electromagnetic energy without mass or charge, emitted by a radionuclide; similar to an X-ray but with higher energy.
Ionising radiation: Radiation that produces ionisation in matter; examples include alpha particles, gamma rays, X-rays and neutrons. When these radiations pass through the tissues of the body, they have sufficient energy to damage the DNA.
Ionisation: The process by which a neutral atom or molecule acquires or loses an electric charge; the production of ions.
Monitoring: The process of searching for the presence of radiation and then measuring, reporting and recording radiation dose rates found within a given area or on a person.
Neutron: A nuclear particle (similar to a proton but without electrical change); emitted during fission and fusion by only a few radionuclides; long range (kilometres) in air and highly penetrating; an external hazard only at detonation; densely ionising.
Non-ionising radiation: Radiation that does not produce ionisation in matter; examples include ultraviolet radiation, light, infrared radiation and radiofrequency radiation. When these radiations pass through the tissues of the body they do not have sufficient energy to damage the DNA directly.
Nuclear Community Charity Fund (NCCF): A charitable organisation for the support of the nuclear community.
Nuclear community: Those affected by nuclear weapons testing internationally.
Radiation weighting factor (RWF): A factor intended to take account of the relative biological effectiveness of different types of radiation according to both their energies and how densely ionising they are.
Radionuclide: An unstable nuclide (atomic nucleus) that emits ionising radiation.
X-ray: A discrete quantity of electromagnetic energy without mass or charge, emitted by an X-ray machine; similar to a gamma ray but with lower energy.
Abbreviations
A: Atomic weight
ABM: Agent Based Modelling
AFRRI: Armed Forces Radiobiology Research Institute
AWE: Atomic Weapons Establishment
BNFL: British Nuclear Fuels Plc
Bq: Becquerel
CA: Cellular Automata
CBRN: Chemical, Biological, Radiological and Nuclear
CCA: Civil Contingencies Act (2004)
CCS: Civil Contingencies Secretariat
COMAH: Control of Major Accident Hazards Regulations (1999)
DEPZ: Detailed Emergency Planning Zone
DNA: Deoxyribonucleic Acid
DSS: Decision Support System
E&W: England and Wales
EPZ: Emergency Planning Zone
ERL: Emergency Reference Level
EU: European Union
GIS: Geographical Information System
PHE: Public Health England
HMNB: Her Majesty’s Naval Base
IAEA: International Atomic Energy Agency
ICRP: International Commission on Radiological Protection
IDW: Inverse Distance Weighting
INES: International Nuclear Event Scale
LRF: Local Resilience Forum
LSOA: Lower Super Output Area
LWR: Light Water Reactor
MAUP: Modifiable Areal Unit Problem
MoD: Ministry of Defence
MYE: Mid-Year Estimate
NAME: Numerical Atmospheric Modelling Environment
NARO: Nuclear Accident Response Organisation
NDA: Nuclear Decommissioning Authority
NI: Nuclear Installation
NII: Nuclear Installations Inspectorate
NIREP: UK Nuclear Industry Road/Rail Emergency Response Plan
NNL: National Nuclear Laboratory
NSD: Nuclear Safety Directorate
OA: Output Area
ONR: Office of Nuclear Regulation
ONS: Office of National Statistics
OS: Ordinance Survey of Great Britain
PACE: Probabilistic Accident Consequence Evaluation
PHE: Public Health England
PITS: Potassium Iodate Tablets
PWR: Pressurised water reactor
RAD: Radiation Absorbed Dose
RCA: Radiation Control Area
REPPIR: (Radiation Emergency Preparedness and Public Information) regulations 2001
RIMNET: Radioactive Incident Monitoring Network
SNI: Sensitive Nuclear Information
Sv: Sievert
THORP: Thermal Oxide Reprocessing Plant, Sellafield
UKAEA: United Kingdom Atomic Energy Authority
UNISDR: United Nations International Strategy for Disaster Reduction
UNSCEAR: United Nations Scientific Committee on the Effects of Atomic Radiation
References and Bibliography
ABC News 2014. Maralinga: Traditional owners given unrestricted access to former nuclear testing site. 5th November 2014. https://mobile.abc.net.au/news/2014-11-05/traditional-owners-given-maralinga-unrestricted-access/5865048?pfm=sm&topic=latest
ACE. 2014. Maralinga’s Afterlife. https://www.theage.com.au/national/maralingas-afterlife-20030511-gdvoq4.html
Agence France Presse. 2014. Marshall Islands want US to resolve unfinished nuclear legacy. 1st March 2014.
Alexis-Martin, B. 2016. Keep the home fires burning: Rekindling the Flame with the French and British Nuclear Test Veterans. University of Southampton Faculty of Social, Human & Mathematical Sciences. 6th July 2016.
Alexis-Martin, B., 2016. “Grapple Slings and Moonshine: Conversations with the men who tested atomic weapons on Christmas Island”. European Research Council Toxic Expertise.
Alexis-Martin, B., 2016. “It was a Blast!’—Camp Life on Christmas Island, 1956–1958”.
Al-Turkait, F. A. and J. U. Ohaeri (2008) “Post-Traumatic Stress Disorder among Wives of Kuwaiti veterans of the First Gulf War.” Journal of Anxiety Disorders 22, 18-31 DOI: http://dx.doi.org/10.1016/j.janxdis.2007.01.011.
Arnold, L. and Pyne, K., 2001. Britain’s Biggest Explosion—Grapple Y. In Britain and the H-Bomb (pp. 165-175). Palgrave Macmillan, London
Arnold, L. and Smith, M., 2006. Britain, Australia and the bomb: The nuclear tests and their aftermath. Springer
Ashley, J. and Hamilton, A., 1991. Nuclear test veterans. Hansard. House of Commons. Official Report, 188(80), pp.375-382
Barnaby, F. and Holdstock, D., 2004. British Nuclear Tests and the Indigenous People of Australia: ROGER CROSS. In The British Nuclear Weapons Programme, 1952-2002 (pp. 93-106). Routledge
Bauer, S., 2018. Radiation Science After the Cold War. The Politics of Measurement, Risk, and Compensation in Kazakhstan. In Health, Technologies, and Politics in Post-Soviet Settings (pp. 225-249). Palgrave Macmillan, Cham
Bauer, S., Gusev, B.I., Pivina, L.M., Apsalikov, K.N. and Grosche, B., 2005. Radiation exposure due to local fallout from Soviet atmospheric nuclear weapons testing in Kazakhstan: solid cancer mortality in the Semipalatinsk historical cohort, 1960–1999. Radiation research, 164(4), pp.409-419.
Bauman, LJ. & Greenberg, E. (1992). “The use of ethnographic interviewing to inform questionnaire construction.” Health Education Quarterly. 19(1), 9-23.
BBC. 2014. Lingering Impact of British Tests on the Australian Outback. British Broadcasting Corporation News. 31st December 2014. https://www.bbc.co.uk/news/world-australia-30640338
BBC. 2018. ‘Nuclear test veteran wants government apology over blasts’. British Broadcasting Corporation. 18th June 2018. Accessed 22nd June 2018 https://www.bbc.co.uk/news/uk-england-derbyshire-44508192
Beck, H.L. and Bennett, B.G., 2002. Historical overview of atmospheric nuclear weapons testing and estimates of fallout in the continental United States. Health Physics, 82(5), pp.591-608
Bergkvist, N.O. and Ferm, R., 2000. Nuclear Explosions 1945-1998 (No. FOA-R–00-01572-180). Defence Research Establishment.
Berkhouse, L., Davis, S.E., Gladeck, F.R., Hallowell, J.H. and Jones, C.B., 1983. Operation DOMINIC I-1962 (No. KT-82-018 (R)). KAMAN TEMPO SANTA BARBARA CA
Bernard, HR. (1988). Research methods in cultural anthropology. Sage Publications.
Bhattacharya, A., 2003. Conceptualising Uyghur separatism in Chinese nationalism. Strategic Analysis, 27(3), pp.357-381
Bien, T.H. and Burge, R., 1990. Smoking and drinking: a review of the literature. International Journal of the Addictions, 25(12), pp.1429-1454.
Black-Branch, J.L. and Fleck, D. eds., 2016. Nuclear Non-Proliferation in International Law-Volume III: Legal Aspects of the Use of Nuclear Energy for Peaceful Purposes. Springer
Boice, J.D., 2017. Epidemiologic Study of One Million US Radiation Workers and Veterans (No. DOE-NCRP-0008944). National Council on Radiation Protection and Measurements, Bethesda, MD (United States).
Bolton, M. 2018. The Devastating Legacy of British and American Nuclear Testing at Kiritimati (Christmas) and Malden Islands. Just Security https://www.justsecurity.org/56127/devastating-legacy-british-american-nuclear-testing-kiritimati-christmas-malden-islands/
Bolton, M., 2017. Humanitarian and Environmental Action to Address Nuclear Harm
Borg, M., 2017. Little known South Australian history: Uncovering the truth behind the nuclear weapons project at Maralinga. Oral History Australia Journal, (39), p.23
Brady, M., 2017. Atomic thunder: The Maralinga story [Book Review]. Aboriginal History, (41), p.235
Briggs, CL. (1986). Learning how to ask: A sociolinguistic appraisal of the role of the interview in social science research. Cambridge University Press.
Britten, N. (1995). “Qualitative Research: Qualitative interviews in medical research.” BMJ. 311: 251-253.
Bromet, E. J., D. Goldgaber, G. Carlson and et al. (2000) “Children’s Well-Being 11 Years after the Chernobyl Catastrophe.” Archives of General Psychiatry 57, 563-571 DOI: 10-1001/pubs.Arch Gen Psychiatry-ISSN-0003-990x-57-6-yoa9231.
Bromet, E. J., J. M. Havenaar and L. Guey (2011) “A 25 Year Retrospective Review of the Psychological Consequences of the Chernobyl Accident.” Clinical Oncology 23, 297-305.
Brown, A.L., 2014. No Promised Land: The Shared Legacy of the Castle Bravo Nuclear Test. Arms Control Today, 44(2), p.40
Brunn, S.D., 2011. Fifty Years of Soviet Nuclear Testing in Semipalatinsk, Kazakstan: Juxtaposed Worlds of Blasts and Silences, Security and Risks, Denials and Memory. In Engineering Earth (pp. 1789-1818). Springer, Dordrecht
Bryant, C., Jackson, H. and Ames, D., 2008. The prevalence of anxiety in older adults: methodological issues and a review of the literature. Journal of affective disorders, 109(3), pp.233-250.
Calhoun, P. S., J. C. Beckham and H. B. Bosworth (2002) “Caregiver Burden and Psychological Distress in Partners of Veterans with Chronic Posttraumatic Stress Disorder.” Journal of Traumatic Stress 15, 205-212.
Card, J. J. (1987) “Epidemiology of PTSD in a National Cohort of Vietnam Veterans.” Journal of Clinical Psychology 43, 6-17.
Care UK Briefing: Health and Care of Older People in England 2017. Accessed 27/06/2018 https://www.ageuk.org.uk/documents/EN-GB/For-professionals/Research/The_Health_and_Care_of_Older_People_in_England_2016.pdf?dtrk=true
Carroll, E. M., D. B. Rueger, D. W. Foy and C. P. Donahoe (1985) “Vietnam Combat Veterans with Posttraumatic Stress Disorder: Analysis of Marital and Cohabitating Adjustment.” Journal of abnormal psychology 94, 329.
Chei, C.L., Lee, J.M.L., Ma, S. and Malhotra, R., 2018. Happy older people live longer. Age and ageing, 47(6), pp.860-866
Chirban, JT. (1996). Interviewing in depth: The interactive relational approach. Thousand Oaks, CA. Sage Publications.
Chitkara, M.G., 1996. Toxic Tibet Under Nuclear China. APH Publishing
Cirincione, J., 2007. Bomb scare: the history and future of nuclear weapons. Columbia University Press
Conard, R.A., 1984. Late radiation effects in Marshall Islanders exposed to fallout 28 years ago. In Radiation carcinogenesis: epidemiology and biological significance
Connell, J., 2012. Population Resettlement in the Pacific: lessons from a hazardous history?. Australian Geographer, 43(2), pp.127-142
Crang, M., 2002. Qualitative methods: the new orthodoxy?. Progress in human geography, 26(5), pp.647-655
Danielssons, P.R., 1986. French Nuclear Colonialism in the Pacific. Ringwood: Penguin Australia.
Darby, S. C., G. M. Kendall, T. P. Fell, J. A. O’Hagan, C. R. Muirhead, J. R. Ennis, A. M. Ball, J. A. Dennis, and R. Doll. 1988. “A summary of mortality and incidence of cancer in men from the United Kingdom who participated in the United Kingdom’s atmospheric nuclear weapon tests and experimental programmes.” Br Med J (Clin Res Ed) 296, no. 6618 (1988): 332-338
Dekel, R. and C. M. Monson (2010) “Military-Related Post-Traumatic Stress Disorder and Family Relations: Current Knowledge and Future Directions.” Aggression and Violent Behavior 15, 303-309 DOI: http://dx.doi.org/10.1016/j.avb.2010.03.001.
Dermott, E. and Gatrell, C. eds., 2018. Fathers, families and relationships: Researching everyday lives. Policy Press
Dictionary.com. (n.d.). “PTSD.” Retrieved 30th May 2016, from http://medical-dictionary.thefreedictionary.com/ptsd.
Dohrenwend, B. P., B. S. Dohrenwend, G. J. Warheit, G. S. Bartlett, R. L. Goldsteen, K. Goldsteen and J. L. Martin (1981) “Stress In The Community: A Report to the President’s Commission on The Accident at Three Mile Island.” Annals of the New York Academy of Sciences 365, 159-174.
Eames, G., 1985. Royal Commission into British Nuclear Tests in Australia: Final submission by counsel on behalf of Aboriginal organisations and individuals
Edwards, D., 2018. Smoking cessation services: how nicotine replacement therapy and counselling through pharmacy can support adherence and quitting. Lung cancer, 15, p.05.
Environment & Society, Autumn, no. 19. Rachel Carson Centre for Environment and Society.
Finlay, WML & Lyons, E. (2001). “Methodological issues in interviewing and using self-report questionnaires with people with mental retardation.” Psychological Assessment. 13(3), 319-335.
Flowerdew, R. and Martin, D. eds., 2005. Methods in human geography: a guide for students doing a research project. Pearson Education
Fontana, A. and Frey, JH. (1994). “Interviewing the art of science” in NK Denzin and YS Lincoln (eds) Handbook of Qualitative Research, pp. 361-376.
Forces Network. 2018. Veteran Who Saw Atomic Bomb Tests Finally Receives MoD Compensation. 28th February 2018. Accessed 22nd June 2018. https://www.forces.net/news/veteran-who-saw-atomic-bomb-tests-finally-receives-mod-compensation
Frankel, M., Scouras, J. and Ullrich, G., 2015. The Uncertain Consequences of Nuclear Weapons Use. JOHNS HOPKINS UNIV LAUREL MD APPLIED PHYSICS LAB
Freedman, L., 1980. Britain and nuclear weapons. Springer
Galovski, T. and J. A. Lyons (2004) “Psychological Sequelae of Combat Violence: A Review of the Impact of PTSD on the Veteran’s Family and Possible Interventions.” Aggression and violent behavior 9, 477-501.
Gelis, U., 2015. ’The Caretaker and the Plague: British Nuclear Weapons Testing in Australia’. Nuclear Age Peace Foundation, 27
Gerrard, M.B., 2015. America’s forgotten nuclear waste dump in the Pacific. SAIS Review of International Affairs, 35(1), pp.87-97
Ghettas, M.L., 2017. Algeria and the Cold War: International Relations and the Struggle for Autonomy. IB Tauris
Gilbert, H., 2013. Indigeneity, time and the cosmopolitics of postcolonial belonging in the Atomic Age. Interventions, 15(2), pp.195-210
Gobo, G. (2008). Introducing Qualitative Methods: Doing ethnography. London, SAGE Publications Ltd
Goodall, H., 1992. ‘The whole truth and nothing but…’: Some intersections of western law, aboriginal history and community memory. Journal of Australian Studies, 16(35), pp.104-119
Gubrium, JA, & Holstein, JA. (2001). Handbook of interview Research: Context and Method. Thousand Oaks, CA. Sage Publications.
Gun, R.T., Parsons, J., Crouch, P., Ryan, P. and Hiller, J.E., 2008. Mortality and cancer incidence of Australian participants in the British nuclear tests in Australia. Occupational and environmental medicine
Gupta, V., 1995. Locating nuclear explosions at the Chinese test site near Lop Nor. Science & Global Security, 5(2), pp.205-244
Hacker, B.C., 1987. The dragon’s tail: radiation safety in the Manhattan Project, 1942-1946. Univ of California Press.
Hacker, B.C., 1992. Radiation safety, the AEC, and nuclear weapons testing. The Public Historian, 14(1), pp.31-53
Hansen, D., & Schriner, C. (2005). Unanswered questions: The legacy of atomic veterans. Health Physics, 89(2), 155–163.
Havenaar, J. M., Rumyantzeva, G.M., van den Brink, W., Poelijoe, N.W., den Bout, J., van Engeland, H. and Koeter, M.W.J. (1997) “Long-term mental health effects of the Chernobyl disaster: an epidemiologic survey in two former Soviet regions.” American Journal of Psychiatry 154, 1605-1607.
Hines, N.O., 1963. Proving ground: an account of the radiobiological studies in the Pacific, 1946-1961. University of Washington Press
Hirshberg, L., 2012. Nuclear families:(Re) producing 1950s suburban America in the Marshall Islands. Organization of American Historians Magazine of History, 26(4), pp.39-43
Hoddinott, P. & Pill, R. (1997). Qualitative research interviewing by general practitioners. A personal view of the opportunities and pitfalls. Family Practice. 14(4), 307-312.
Hoey, B.A., 2014. A simple introduction to the practice of ethnography and guide to ethnographic fieldnotes. Marshall University Digital Scholar, 2014, pp.1-10.
Holroyd-Leduc, J., Resin, J., Ashley, L., Barwich, D., Elliott, J., Huras, P., Légaré, F., Mahoney, M., Maybee, A., McNeil, H. and Pullman, D., 2016. Giving voice to older adults living with frailty and their family caregivers: engagement of older adults living with frailty in research, health care decision making, and in health policy. Research involvement and engagement, 2(1), p.23.
Hooper, R., Rona, R.J., Jones, M., Fear, N.T., Hull, L. and Wessely, S., 2008. Cigarette and alcohol use in the UK Armed Forces, and their association with combat exposures: a prospective study. Addictive behaviors, 33(8), pp.1067-1071.
Hotez, P.J., 2016. Neglected tropical diseases in the anthropocene: the cases of Zika, Ebola, and other infections. PLoS neglected tropical diseases, 10(4), p.e0004648
IPPNW International Commission to Investigate the Health, Environmental Effects of Nuclear Weapons Production, Institute for Energy, Environmental Research (Takoma Park and Md.), 1991. Radioactive heaven and earth: the health and environmental effects of nuclear weapons testing in, on, and above the earth. Apex Pr.
Japan Times. 2012. China Nuclear Tests Prompt Uighur Campaign. 9th August 2012 https://www.japantimes.co.jp/news/2012/08/09/national/china-nuclear-tests-prompt-uighur-campaign/#.W9h92Hv7Spo
Johnston, B.R., 2010. Social responsibility and the anthropological citizen. Current Anthropology, 51(S2), pp.S235-S247
Jones, C.G., 2005. A review of the history of US radiation protection regulations, recommendations, and standards. Health physics, 88(2), pp.105-124.
Jorgenson, T. 2016. Bikini islanders still deal with fallout of US nuclear tests, 70 years later. The Conversation. June 29th 2016. https://theconversation.com/bikini-islanders-still-deal-with-fallout-of-us-nuclear-tests-70-years-later-58567
Jorgenson. D, 1989, ‘The methodology of participant observation’, in Participant observation, Applied Social Research Methods, SAGE Publications, Inc., Thousand Oaks, CA, pp. 12-25
Kahn, M., 2000. Tahiti intertwined: Ancestral land, tourist postcard, and nuclear test site. American Anthropologist, 102(1), pp.7-26.
Kassenova, T., 2016. Banning nuclear testing: lessons from the Semipalatinsk nuclear testing site. The Nonproliferation Review, 23(3-4), pp.329-344
Kawano, N., Hirabayashi, K., Matsuo, M., Taooka, Y., Hiraoka, T., Apsalikov, K.N., Moldagaliev, T. and Hoshi, M., 2006. Human suffering effects of nuclear tests at Semipalatinsk, Kazakhstan: established on the basis of questionnaire surveys. Journal of radiation research, 47(SupplementA), pp.A209-A217
Keane, J., 2003. Maralinga’s Afterlife. Feature Article. The Age, 11
Keown, M., Taylor, A. and Treagus, M. eds., 2018. Anglo-American Imperialism and the Pacific: Discourses of Encounter. Routledge
Kessler, R. C., A. Sonnega, E. Bromet, M. Hughes and C. B. Nelson (1995) “Posttraumatic Stress Disorder in the National Comorbidity Survey.” Archives of General Psychiatry 52, 1048-1060.
Khalturin, V.I., Rautian, T.G., Richards, P.G. and Leith, W.S., 2005. A review of nuclear testing by the Soviet Union at Novaya Zemlya, 1955–1990. Science and Global Security, 13(1-2), pp.1-42
Kuletz, V., 2001. Invisible spaces, violent places: Cold War nuclear and militarized landscapes. Violent environments, pp.237-260.
Kuletz, V.L., 2016. The tainted desert: Environmental and social ruin in the American West. Routledge
Kunkle, T. and Ristvet, B., 2013. CASTLE BRAVO: Fifty Years of Legend and Lore. A Guide to Off-Site Radiation Exposures(No. DTRIAC-SR-12-001). Defense threat reduction information analysis center kirtland AFB NM
Kvale, S. (1983). The qualitative research interview: A phenomenological and hermeneutical mode of understanding. Journal of Phenomenological Psychology. 14(2), 171-196.
Kvale, S. (1996). InterViews: An Introduction to Qualitative Research Interviewing. Thousand Oaks, CA: Sage Publications.
Langham, W.H. and Healy, J.W., 1973. Maximum permissible body burdens and concentrations of plutonium: Biological basis and history of development. In Uranium· Plutonium Transplutonic Elements (pp. 569-592). Springer, Berlin, Heidelberg.
Lokan, K.H., 1985. Residual radioactive contamination at Maralinga and Emu, 1985 (No. ARL/TR–070). Australian Radiation Lab.
Maclellan, N., 2005. The nuclear age in the Pacific islands. The Contemporary Pacific, pp.363-372
Maclellan, N., Deery, P. and Kimber, J., 2015, February. Grappling with the Bomb: Opposition to Pacific nuclear testing in the 1950s. In Proceedings of the 14th Biennial Labour History Conference (p. 21). Australian Society for the Study of Labour History
Makhijani, A., Hu, H. and Yih, K. eds., 2000. Nuclear wastelands: a global guide to nuclear weapons production and its health and environmental effects. MIT Press.
Maralinga Tours Website title page “Maralinga Tours – discover Australia’s shocking atomic legacy” https://maralingatours.com.au
Mattingley, C. and Hampton, K., 1988. Survival in our own land:” Aboriginal” experiences in” South Australia” since 1836. Wakefield Press Pty, Limited
Mayor, S., 2017. Older patients with mental illness are less likely to be referred, study finds. BMJ: British Medical Journal (Online), 357.
McCormack, L., S. White and J. Cuenca (2016) “A Fractured Journey of Growth: Making Meaning of a ‘Broken’ Childhood and Parental Mental Ill-Health.” Community, Work & Family, 1-19 DOI: 10.1080/13668803.2015.1117418.
McCracken, G. (1998). The Long Interview. Newbury Park, CA: Sage Publications.
McLaughlin, R., Nielsen, L. and Waller, M., 2008. An evaluation of the effect of military service on mortality: quantifying the healthy soldier effect. Annals of epidemiology, 18(12), pp.928-936
Meier, E.A., Gallegos, J.V., Thomas, L.P.M., Depp, C.A., Irwin, S.A. and Jeste, D.V., 2016. Defining a good death (successful dying): literature review and a call for research and public dialogue. The American Journal of Geriatric Psychiatry, 24(4), pp.261-271
Mental Health Foundation. (n.d.). “Armed Forces and Mental Health.” Retrieved 11th May 2016, from https://www.mentalhealth.org.uk/a-to-z/a/armed-forces-and-mental-health.
Menvielle, G., Fayossé, A., Radoï, L., Guida, F., Sanchez, M., Carton, M., Cyr, D., Schmaus, A., Cénée, S., Fevotte, J. and Delafosse, P., 2016. The joint effect of asbestos exposure, tobacco smoking and alcohol drinking on laryngeal cancer risk: evidence from the French population-based case–control study, ICARE. Occup Environ Med, 73(1), pp.28-33
Michel, D., 2003. Villains, victims and heroes: Contested memory and the British nuclear tests in Australia. Journal of Australian Studies, 27(80), pp.221-228
Miles, R., S. Green, G. Mynors and J. Suppiah (2011) “British Nuclear Test Veterans Health Needs Audit.”
Mittmann, J.D., 2017. Maralinga: Aboriginal poison country. Agora, 52(3), p.25
Mix, T.L., Cable, S. and Shriver, T.E., 2009. Social control and contested environmental illness: the repression of III nuclear weapons workers. Human Ecology Review, pp.172-183.
Mody, Lona, Douglas K. Miller, Joanne M. McGloin, Marcie Freeman, Edward R. Marcantonio, Jay Magaziner, and Stephanie Studenski. “Recruitment and Retention of Older Adults in Aging Research: (See editorial comments by Dr. Stephanie Studenski, pp 2351–2352).” Journal of the American Geriatrics Society 56, no. 12 (2008): 2340-2348
Monden, R., Rosmalen, J. and Creed, F., 2018. The risk factors for new onsets of Irritable Bowel Syndrome, Chronic Fatigue Syndrome and Fibromyalgia: The Lifelines study. Journal of Psychosomatic Research, 109, p.120.
Muirhead, C. R., D. Bingham, R. G. E. Haylock, J. A. O’hagan, A. A. Goodill, G. L. C. Berridge, M. A. English, N. Hunter, and G. M. Kendall. 2003. “Follow up of mortality and incidence of cancer 1952–98 in men from the UK who participated in the UK’s atmospheric nuclear weapon tests and experimental programmes.” Occupational and environmental medicine 60, no. 3 (2003): 165-172
Muirhead, C.R., Kendall, G.M., Darby, S.C., Doll, R., Haylock, R.G.E., O’Hagan, J.A., Berridge, G.L.C., Phillipson, M.A. and Hunter, N., 2004. Epidemiological studies of UK test veterans: II. Mortality and cancer incidence. Journal of Radiological Protection, 24(3), p.219
Nesipbaeva, K. and Chang, C., Environmental problems on Kazakhstan and the Nevada-Semipalatinsk antinuclear movement. IAEA report.
Nobody Told Us Anything…The title of a film commissioned by BNTVA and produced by Charles Stewart http://www.bbfc.co.uk/releases/nobody-told-us-anything-2014
Norris, R.S. and Arkin, W.M., 1998. Soviet Nuclear Testing, August 29, 1949-October 24, 1990. Bulletin of the Atomic Scientists, 54(3), p.69
Olfson M, Marcus SC, Druss B, et al. National trends in the outpatient treatment of depression. JAMA. 2002;287:203–209. [PubMed]
ONS. 2017. Adult smoking habits in the UK: 2015. National Smoking Survey. Office of National Statistics.
Oulton, W.E., 1987. Christmas Island Cracker: An Account of the Planning and Execution of the British Thermo-nuclear Bomb Tests, 1957. Thomas Harmsworth Publishing
Oulton, W.E., 1987. Christmas Island Cracker: An Account of the Planning and Execution of the British Thermo-nuclear Bomb Tests, 1957. Thomas Harmsworth Publishing
Parkinson, A., 2002. Articles on the Maralinga ‘clean-up’ by nuclear engineer and whistle-blower Alan Parkinson. Journal of the International Physicians for the Prevention of Nuclear War, 7(2), pp.77-81
Parkinson, A., 2004. The Maralinga rehabilitation project. Medicine, Conflict an Survival, 20(1), pp.70-80
Parsons, K.M. and Zaballa, R.A., 2017. Bombing the Marshall Islands: A Cold War Tragedy. Cambridge University Press
Patel, M.X., Doku, V. and Tennakoon, L., 2003. Challenges in recruitment of research participants. Advances in Psychiatric Treatment, 9(3), pp.229-238
Phelan, J. C., E. J. Bromet and B. G. Link (1998) “Psychiatric Illness and Family Stigma.” Schizophrenia Bulletin 24, 115-126.
Power, P.F., 1986. The South Pacific Nuclear-Weapon-Free Zone. Pacific Affairs, pp.455-475
Prăvălie, R., 2014. Nuclear weapons tests and environmental consequences: a global perspective. Ambio, 43(6), pp.729-744
Purvis‐Roberts, K.L., Werner, C.A. and Frank, I., 2007. Perceived risks from radiation and nuclear testing near Semipalatinsk, Kazakhstan: A comparison between physicians, scientists, and the public. Risk Analysis: An International Journal, 27(2), pp.291-302
Pyne, K., 1995. Art or article? The need for and nature of the British hydrogen bomb, 1954–58. Contemporary British History, 9(3), pp.562-585
Pyne, K., 1995. Art or article? The need for and nature of the British hydrogen bomb, 1954–58. Contemporary British History, 9(3), pp.562-585
Roff, S. U. E. “Establishing the possible radiogenicity of morbidity and mortality from participation in UK nuclear weapons development.” Medicine, Conflict and Survival 20, no. 3 (2004): 218-241
Rabionet, S.E., 2011. How I learned to design and conduct semi-structured interviews: An ongoing and continuous journey. The Qualitative Report, 16(2), p.563.
Radiation Exposure Compensation Act https://www.ncbi.nlm.nih.gov/books/NBK221729/
Ray, S. L. and M. Vanstone (2009) “The impact of PTSD on Veterans’ Family Relationships: An Interpretative Phenomenological Inquiry.” International Journal of Nursing Studies 46, 838-847.
Reed, T.C. and Stillman, D.B., 2010. The nuclear express: A political history of the bomb and its proliferation. Zenith Press.
Riggs, D. S., C. A. Byrne, F. W. Weathers and B. T. Litz (1998) “The Quality of the Intimate Relationships of Male Vietnam Veterans: Problems Associated with Posttraumatic Stress Disorder.” Journal of Traumatic Stress 11, 87-101.
Rivas, M., Rojas, E., Araya, M.C. and Calaf, G.M., 2015. Ultraviolet light exposure, skin cancer risk and vitamin D production. Oncology letters, 10(4), pp.2259-2264
Roberts, B., Manning, R.A. and Montaperto, R.N., 2000. China: the forgotten nuclear power. Foreign Aff., 79, p.53
Roberts, S., 2012. Imaginary terrorism? The global war on terror and the narrative of the Uyghur terrorist threat. The Institute for European, Russian and Eurasian Studies (IERES), Elliott School of International Affairs
Robinette, C.D., Jablon, S. and Preston, T.L., 1985. Mortality of Nuclear Weapons Test Participants. NATIONAL RESEARCH COUNCIL WASHINGTON DC COMMISSION ON LIFE SCIENCES
Roff, S.R., 1998. Puff the magic dragon: how our understanding of fallout, residual and induced radiation evolved over fifty years of nuclear weapons testing. Medicine, Conflict and Survival, 14(2), pp.106-119
Roff, S.R., 1999. Mortality and morbidity of members of the British Nuclear Tests Veterans Association and the New Zealand Nuclear Tests Veterans Association and their families. Medicine, conflict, and survival, 15, pp.i-ix
Roff, S.R., 2004. Long-term health effects in UK test veterans. In The British Nuclear Weapons Programme, 1952-2002 (pp. 117-138). Routledge.
Rubin, HJ., Rubin, IS. (2004). Qualitative interviewing: The art of hearing data. 2nd Edition. Thousand Oaks, CA. Sage Publications.
Ruff, T.A., 2015. The humanitarian impact and implications of nuclear test explosions in the Pacific region. International Review of the Red Cross, 97(899), pp.775-813
Sagan, S.D., 1997. Why do states build nuclear weapons? Three models in search of a bomb. International security, 21(3), pp.54-86.
Schwartz, S.I., 2011. Atomic audit: the costs and consequences of US nuclear weapons since 1940. Brookings Institution Press
Scope. 2018. Disability Facts and Figures. Retrieved 11th April 2018. https://www.scope.org.uk/media/disability-facts-figures
Shichor, Y., 2015. See No Evil, Hear No Evil, Speak No Evil: Middle Eastern Reactions to Rising China’s Uyghur Crackdown. Griffith Asia Quarterly, 3(1), pp.62-85
Siracusa, J.M., 2008. Nuclear weapons: a very short introduction. OUP Oxford
Spradley, JP. (1979) The Ethnographic Interview. Holt, Reinhart and Winston.
Stawkowski, M.E., 2016. “I am a radioactive mutant”: Emergent biological subjectivities at Kazakhstan’s Semipalatinsk Nuclear Test Site. American Ethnologist, 43(1), pp.144-157
Stillwell, M. C. (2015). Cultivating Partnerships Between Community Leaders and Service Agencies to Provide Support for Military Families.
Susanne Bauer, Boris I. Gusev, Ludmila M. Pivina, Kazbek N. Apsalikov and Bernd Grosche (2005) Radiation Exposure Due to Local Fallout from Soviet Atmospheric Nuclear Weapons Testing in Kazakhstan: Solid Cancer Mortality in the Semipalatinsk Historical Cohort, 1960-1999 Radiation Research Vol. 164, No. 4, Part pp. 409-419
Tang, F.R., 2017. Low Dose/Dose Rate Radiation Exposure and Human Mental Health. EC Psychology and Psychiatry, 6, pp.56-59.
Taylor, J., 2011. Postcolonial transformation of the Australian Indigenous population. Geographical Research, 49(3), pp.286-300
Tharmalingam, S., Sreetharan, S., Kulesza, A.V., Boreham, D.R. and Tai, T.C., 2017. Low-dose ionizing radiation exposure, oxidative stress and epigenetic programing of health and disease. Radiation research, 188(4.2), pp.525-538
The Guardian. 2016. Marshall Islands nuclear arms lawsuit thrown out by UN’s top court. 6th October 2016. https://www.theguardian.com/world/2016/oct/06/marshall-islands-nuclear-arms-lawsuit-thrown-out-by-uns-top-court
Threet, J.B., 2005. Testing the Bomb: Disparate Impacts on Indigenous Peoples in the American West, the Marshall Islands, and in Kazakhstan. U. Balt. J. Envtl. L., 13, p.29
Titus, A.C., 2001. Bombs in the backyard: atomic testing and American politics (No. 25). University of Nevada Press
Toptayeva, B., 2018. Antinuclear movements in the US and Kazakhstan: A cross-cultural analysis of mass communication patterns. Iowa State University Thesis Repository.
Tóth, T., 2016. Conflict, cooperation, and the Comprehensive Nuclear-Test-Ban Treaty: financial markets as a metaphor for cycles in global security. The Nonproliferation Review, 23(3-4), pp.377-384
Trundle, C. (2011) “Biopolitical Endpoints: Diagnosing a Deserving British Nuclear Test Veteran.” Social Science & Medicine 73, 882-888 DOI: http://dx.doi.org/10.1016/j.socscimed.2011.05.034.
Trundle, C. and Scott, B.I., 2013. Elusive genes: Nuclear test veterans’ experiences of genetic citizenship and biomedical refusal. Medical anthropology, 32(6), pp.501-517.
Trundle, C., 2011. Biopolitical endpoints: Diagnosing a deserving British nuclear test veteran. Social Science & Medicine, 73(6), pp.882-888.#
United Nations. Scientific Committee on the Effects of Atomic Radiation, 2008. Report of the United Nations Scientific Committee on the Effects of Atomic Radiation: Fifty-sixth Session (10-18 July 2008) (No. 46). United Nations Publications.
Van Beugen, S., Ferwerda, M., Hoeve, D., Rovers, M.M., Spillekom-van Koulil, S., van Middendorp, H. and Evers, A.W., 2014. Internet-based cognitive behavioral therapy for patients with chronic somatic conditions: a meta-analytic review. Journal of medical Internet research, 16(3).
Verbrugge, L.M. and Yang, L.S., 2002. Aging with disability and disability with aging. Journal of disability policy studies, 12(4), pp.253-267.
Vogt, D. S., A. P. Pless, L. A. King and D. W. King (2005) “Deployment Stressors, Gender, and Mental Health Outcomes among Gulf War I Veterans.” Journal of Traumatic Stress 18, 115-127.
Walsh, J., 1997. Surprise down under: The secret history of Australia’s nuclear ambitions. The Nonproliferation Review, 5(1), pp.1-20
Warren, CAB., Karner, TX. (2005). Discovering qualitative methods: Field research, interviews and analysis. Los Angeles, CA, Roxbury Publishing Company.
Wegmarshaus, G.R., 2018. Nuclear Power and Civil Society in Post-Soviet Russia. In Nuclear Energy And Security In The Former Soviet Union (pp. 99-119). Routledge
Weisgall, J.M., 1980. The nuclear nomads of Bikini. Foreign Policy, (39), pp.74-98
Williams, G.A., O’Brien, R.S., Grzechnik, M. and Wise, K.N., 2017. Estimates Of Radiation Doses To The Skin For People Camped At Wallatinna During The Uk Totem 1 Atomic Weapons Test. Radiation protection dosimetry, 174(3), pp.322-336
Wise, K.N. and Moroney, J.R., 1992. Public health impact of fallout from British nuclear weapons tests in Australia, 1952-1957 (No. ARL-TR–105). Australian Radiation Lab
Zaretsky, N., 2015. Radiation Suffering and Patriotic Body Politics in the 1970s and 1980s. Journal of Social History, 48(3), pp.487-510
[1] The title of a film commissioned by BNTVA and produced by Charles Stewart http://www.bbfc.co.uk/releases/nobody-told-us-anything-2014
[2] The authors would like to thank the Old BNTVA for supporting our attendance.
[3] This understanding was developed from conversation with BNTVA committee standard bearer, who undertakes funereal duties.




{kind=link}